



Studies on serum IgE levels during pregnancy are limited.
ObjectiveTo investigate the course of serum total IgE levels during pregnancy and postpartum.
Methods159 pregnant subjects provided 218 serum samples during various stages of pregnancy and the postpartum period. Serum total IgE geometric means were compared at various trimesters and postpartum. In addition, the postpartum IgE data were analysed according to the method of delivery. Analysis was also done according to history of allergy.
ResultsThe geometric mean serum total IgE was 20.5 IU/ml in the first trimester, 20.8 IU/ml in the second and 22.2 IU/ml in the third. Postpartum serum IgE level showed a lower mean, 14.9 IU/ml during the early postpartum period (less than 30 days) compared to 30.3 IU/ml during the late postpartum period (30 days-25 weeks). However this was not statistically significant. Serum IgE in the postpartum period also did not differ according to method of delivery. A history of allergy was positive in 98 samples, negative in 61 and unclear in 59. Using analysis of variance, none of these three groups showed significant change in serum total IgE level during pregnancy or postpartum.
ConclusionIn this cross-sectional study, serum total IgE levels showed no statistically significant changes during pregnancy or postpartum. This finding would be of greater weight if reproduced in a larger number of subjects with multiple serial samples at fixed regular time intervals during pregnancy and postpartum.
Pregnancy is associated with several physiological, hormonal and immunological changes. Studies on serum immunoglobulin levels are limited in number and showed conflicting findings. Reports show that the levels of IgG did not change1–3 or decreased significantly.4–9 The fall in serum IgG levels may be attributed to the haemodilution during pregnancy and transplacental transfer of maternal IgG to the fetus.10 Serum IgA was shown to have no change,1,3,5,9 decreased4,8 or increased.7 Similarly, serum IgM was shown to have no change,1,3,5,9 decreased4,8 or increased.7
Serum total IgE level is often used in allergy practice as a general marker of atopy, although it is neither inclusive nor exclusive. However, the basal serum total IgE level in health is influenced to varying degrees by numerous factors including genetics, age, race, season, mode of infant feeding and tobacco smoking.11 Studies on the effect of pregnancy on serum total IgE are limited. Serum IgE was shown to have no change,10,12 decreased,13 or slightly increased.14 Pregnant asthmatics who had increasing or unchanged IgE were shown to have a tendency for asthma exacerbations.15 Most of these studies were based on a relatively small number of subjects and did not use logarithmic transfer of IgE level in the statistical analysis. One study16 reported a slight increase in total IgE levels at one month postpartum compared to the third trimester, but did not include samples during the first or second trimester.
The objective of our study was to look for any quantitative changes in serum total IgE level during different stages of pregnancy and the postpartum period.
MethodsThe study was approved by the Institutional Review Board at Louisiana State University Medical Center. Pregnant women attending prenatal clinics and undergoing routine blood tests were informed of the study. If a written consent was obtained, the left-over serum samples were collected whenever the subject underwent routine blood test during pregnancy and after delivery. Parental consent is not required for pregnant subjects under 18 years of age. The serum samples were then stored at -4°C for later measurement of total IgE level. A total of 159 pregnant women (age 15-39 years, mean 24.2 years) provided a total of 218 serum samples; 162 during pregnancy and 56 postpartum. All serum samples were collected from healthy subjects. In 98 (44.9%) of samples, the donor had a history of allergy defined as a physician-diagnosed or a strong medical history compatible with allergic rhinitis, asthma, urticaria, angio-oedema, atopic eczema, or systemic anaphylaxis.
Statistical analysisThe IgE data were analysed using logarithms. Trends of change in IgE level were examined by comparing the geometric means at various trimesters and postpartum. Since the samples were mostly from different women, the study is primarily cross-sectional. Student's t-test was used to compare two means17 and analysis of variance was used to assess the variation between more than two means.18 In addition to the time variable, the postpartum IgE data were analysed according to the method of delivery; vaginal versus caesarean section. Analysis was also done according to the history of allergy.
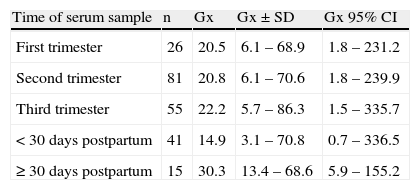
ResultsSerum IgE level during pregnancy and postpartumOf the 218 serum samples obtained, 26 were during the first trimester, 81 during the second, 55 during the third, and 56 were during the first 25 weeks after delivery. The concentration of serum IgE showed no statistically significant variation during pregnancy. The geometric mean serum IgE was 20.5 IU/ml in the first trimester, 20.8 IU/ml in the second, and 22.2 IU/ml in the third (Table 1). Postpartum serum IgE level showed a lower mean, 14.9 IU/ml during the early postpartum period (less than 30 days) compared to 30.3 IU/ml during the late postpartum period (30 days-25 weeks). However this was not statistically significant, probably due to the small number of samples. The 56 postpartum sera were available from 45 women; 30 whose delivery was by caesarean section with a mean IgE level of 15.1 IU/ml, which was similar to that in the 15 women who had normal vaginal delivery of 17.5 IU/ml. Understandably, follow-up visits and postpartum blood drawing was more in women whose delivery was by caesarean section.
Total IgE level in 218 serum samples from 159 subjects during pregnancy and postpartum.
| Time of serum sample | n | Gx | Gx±SD | Gx 95% CI |
| First trimester | 26 | 20.5 | 6.1 – 68.9 | 1.8 – 231.2 |
| Second trimester | 81 | 20.8 | 6.1 – 70.6 | 1.8 – 239.9 |
| Third trimester | 55 | 22.2 | 5.7 – 86.3 | 1.5 – 335.7 |
| < 30 days postpartum | 41 | 14.9 | 3.1 – 70.8 | 0.7 – 336.5 |
| ≥ 30 days postpartum | 15 | 30.3 | 13.4 – 68.6 | 5.9 – 155.2 |
Gx=geometric mean in IU/ml; SD=standard deviation; CI=confidence interval.
Seven subjects had multiple serum samples drawn throughout their course of pregnancy and postpartum period (Fig. 1). Serum IgE levels remained almost unchanged except in two subjects; one (DM) had a sharp decline early in pregnancy and a slower decline following delivery, and the other (DS) showed a sharp serum IgE rise in the early postpartum period.
Serum IgE in subjects according to history of allergy
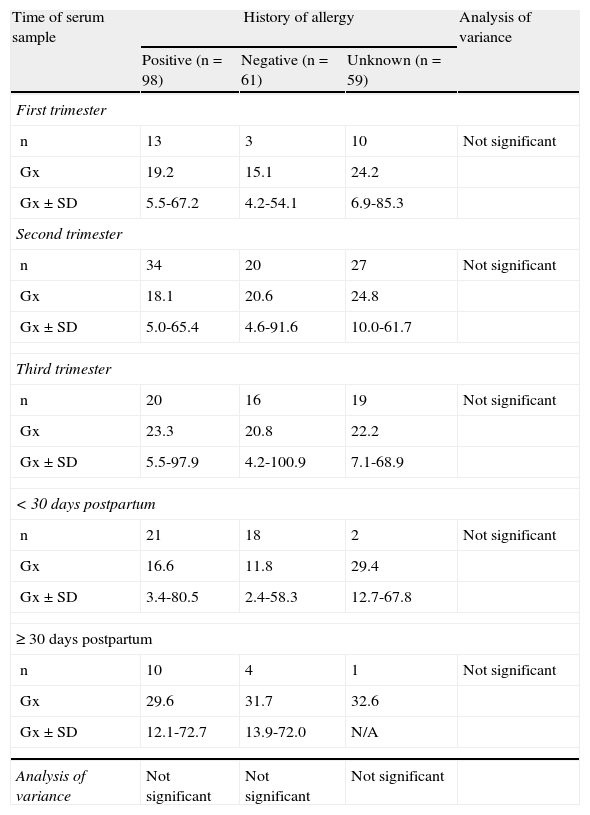
A history of allergy was positive in 98 instances, negative in 61 and unclear in 59. Using analysis of variance, none of the three groups showed significant change in serum IgE level during pregnancy or postpartum. Also, these three groups did not differ among themselves at any trimester or postpartum period (Table 2)
Total IgE level in 218 serum samples from 159 subjects during pregnancy and postpartum according to history of allergy.
| Time of serum sample | History of allergy | Analysis of variance | ||
| Positive (n=98) | Negative (n=61) | Unknown (n=59) | ||
| First trimester | ||||
| n | 13 | 3 | 10 | Not significant |
| Gx | 19.2 | 15.1 | 24.2 | |
| Gx±SD | 5.5-67.2 | 4.2-54.1 | 6.9-85.3 | |
| Second trimester | ||||
| n | 34 | 20 | 27 | Not significant |
| Gx | 18.1 | 20.6 | 24.8 | |
| Gx±SD | 5.0-65.4 | 4.6-91.6 | 10.0-61.7 | |
| Third trimester | ||||
| n | 20 | 16 | 19 | Not significant |
| Gx | 23.3 | 20.8 | 22.2 | |
| Gx±SD | 5.5-97.9 | 4.2-100.9 | 7.1-68.9 | |
| < 30 days postpartum | ||||
| n | 21 | 18 | 2 | Not significant |
| Gx | 16.6 | 11.8 | 29.4 | |
| Gx±SD | 3.4-80.5 | 2.4-58.3 | 12.7-67.8 | |
| ≥ 30 days postpartum | ||||
| n | 10 | 4 | 1 | Not significant |
| Gx | 29.6 | 31.7 | 32.6 | |
| Gx±SD | 12.1-72.7 | 13.9-72.0 | N/A | |
| Analysis of variance | Not significant | Not significant | Not significant | |
Gx=geometric mean in IU/ml; SD=standard deviation.
The comparison is both vertical (according to time) and horizontal (according to history of allergy).
In this cross-sectional study, we found that the serum total IgE level did not significantly change during pregnancy. Multiple serial samples were available on a small number of subjects and did not show any specific trend of change. This finding would be of greater weight if reproduced in a larger number of subjects with multiple serial samples at fixed regular time intervals during pregnancy and postpartum.
In a limited study, Gluck and Gluck15 studied the changes of serum IgE and asthma during pregnancy in 17 women compared with six controls without asthma. In the asthmatic group, serum IgE increased in six subjects, decreased in seven and was unchanged in four. All six subjects without asthma in the control group had decreased serum IgE. They noted that subjects with an increased or unchanged IgE have a tendency for their asthma to worsen during pregnancy. In our series, mean serum total IgE level during early postpartum was lower (14.9 IU/ml) than during the third trimester (22.2 IU/ml). A recent study19 found that total IgE levels were higher during early pregnancy than one year postpartum in 13 allergic subjects but not in 30 non-allergic subjects. Our study found no relationship between history of allergy and changes in serum total IgE during pregnancy or postpartum. It has been reported that maternal IgE are present on foetal macrophages in the placental villous tissue irrespective of maternal allergy status.20
Eskild et al.21 reported no significant association between IgE levels in the first or second trimester and the risk of subsequent preeclampsia. Placental trophoblasts were studied regarding immunoglobulins attached to the cell membrane.22 IgG was observed on the syncytial cytotrophoblastic cell membrane, cytoplasm and nucleus in all stages of gestation. IgE was absent from the villi of placental tissue obtained from therapeutic abortions, induced labour, and elective caesarean section. IgE was present on the surface of the trophoblast in trace amounts in toxaemia of pregnancy and in moderate amounts in spontaneous labour at full term. The author postulated that the latter finding might offer a possible explanation for initiating normal labour through an IgE-mediated inflammatory reaction as proposed by Larsh23 for the mechanism of expulsion of intestinal parasites. Since we found no significant changes in serum IgE level during pregnancy or postpartum, if IgE has a role in initiating labour, the effect might be locally at the syncytial cytotrophoblastic cell level. Currently, the role of IgE in the placenta remains unknown.24
We noted that serum total IgE level was lower, although not statistically significant, during the early postpartum period compared to the third trimester (14.9 vs 22.2 IU/ml) or compared with late postpartum (14.9 vs 30.3 IU/ml). A study by Landesman and Miller25 revealed that plasma volume rises in the postpartum period and reaches maximum in 72-96hours. It returns to the normal non-pregnant range 3-4 weeks after delivery. The reasons for these plasma volume changes are not clear, but it could be at least partly a result of administration of intravenous fluids during labour for replacing blood loss. Our findings of reduced IgE level may be due to the increase in plasma volume and haemodilution during the early postpartum period. It is unlikely to be due to hormonal changes because serum IgE has been found to have no correlation with sex hormone levels.14
A study by Perry et al.16 showed a very slight increase (average 5 IU/ml) of serum total IgE in the postpartum period at one month and at one year compared to the level during the third trimester. That study, however, did not include samples during various times of pregnancy. The authors postulated that haemodilution during pregnancy might have played a role in lowering the IgE levels during the third trimester of pregnancy. When estimated plasma volume changes were applied to the data, the authors found the difference in total IgE levels before and one month after delivery to be negligible.
In conclusion, our study revealed no significant changes in serum total IgE levels during pregnancy or postpartum period. Our finding would be better confirmed by a study of multiple serial samples drawn at fixed time intervals.
