


Respiratory viral infections are a major cause of hospitalisation in infants <1 year and might cause severe symptoms in preterm infants. Our aim was to analyse admissions due to respiratory infections in moderate, late and term infants, and to identify risk factors for hospitalisation in preterm versus term.
MethodsProspective study in a cohort of moderate and late preterm, and term infants born between October/2011 and December/2012. Admissions due to respiratory infections during the first year of life were analysed and compared among moderate (32–33), late (34–36) and term infants. Sixteen respiratory viruses were detected by RT-PCR. Clinical data were collected.
Results30 (20.9%) out of 143 preterm infants required admission for respiratory infection, versus 129 (6.9%) of 1858 term infants born in the same period (p<0.0001, OR: 3.6 CI 2.0 to 5.0). Hospitalised children had a higher prevalence of hyaline membrane disease (HMD) at birth (p<0.001, OR: 7.7 CI: 2.121 to 27.954) and needed more mechanical ventilation (p<0.001, OR: 5.7 CI: 1.813 to 18.396). Virus was identified in 25/30 (83%) preterm babies, and in 110/129 (85%) term infants. The most frequent viruses in preterm infants were RSV (76%) rhinovirus (20%). Clinical and epidemiological characteristics among term and preterm infants were similar.
ConclusionsThe risk of respiratory admissions during the first year of life is up to 3.6 times higher in moderate and late preterm. Once admitted, clinical features of respiratory episodes requiring hospitalisation are similar among term and preterm infants. Hyaline membrane disease and mechanical ventilation were also risk factors for respiratory admissions.
Respiratory tract viral infection continues to be among the most common reasons for visits to the emergency department and hospitalisation in children, particularly in the case of infants younger than one year. These infections can cause severe symptoms in preterm infants, such as respiratory distress with high morbidity and mortality. Lower respiratory viral infections (LRTI), especially due to respiratory syncytial virus (RSV), are the leading cause of hospital admissions among infants.1 Having a history of prematurity (less than 32 weeks of gestational age) is a risk factor for severe LRTI in early childhood, and late preterm babies have been considered in the same risk group.2 Nevertheless, this issue is under investigation and some research groups have not found a higher risk in late preterm infants (more than 336 weeks of gestational age (GA).3 Respiratory distress syndrome at birth could be a risk factor for hospitalisation in this group.4 Other authors have not found association between prematurity and hospitalisation during the first two years of life.5
Throughout the years, clinicians have considered respiratory syncytial virus followed by influenza as the most common pathogens responsible for respiratory infections. Over the past decade, new viruses have been discovered through more specific testing. This includes human metapneumovirus (HMPV), rhinovirus (RV), human bocavirus (HBoV) and others.6
We designed a prospective study in a cohort of moderate-late preterm and term infants. Our aim was to evaluate incidence and clinical characteristics of hospitalisation due to respiratory tract infections associated to a panel of 16 different respiratory viruses during the first year of life.
Patients and methodsThis was a systematic prospective study conducted at Severo Ochoa Hospital (Leganes, Madrid, Spain) to assess the incidence, epidemiology and clinical characteristics of respiratory viral infections that needed hospitalisation in a cohort of moderate and late preterm infants during the first year of life. 143 preterm infants born between 320 and 366 weeks were followed up by phone, and hospitalisation incidence due to respiratory viral infections was compared with the 1858 term babies born during the same period in our hospital. The enrolment period was October 2011 to December 2012. The study was funded by FIS (Fondo de Investigaciones Sanitarias – Spanish Health Research Fund) Grant 09/00246 and approved by The Medical Ethics Committee. Parents were informed and consent was obtained.
Clinical assessmentPatients hospitalised due to respiratory symptoms were evaluated by an attending physician. During the hospital stay, and as part of the study, a physician filled out a study-questionnaire with the following variables: age, sex, clinical diagnosis, history of prematurity and underlying chronic diseases, need for oxygen therapy assessed by transcutaneous oxygen saturation, axillary temperature ≥38°C, presence of infiltrates/atelectasis in radiographs, administration of antibiotic therapy, duration of hospital stay, total white blood cell (WBC) count, C-reactive protein (CRP) serum values, and result of blood culture if performed. Oxygen therapy was provided in order to achieve oxygen saturation ≥94%.
Upper respiratory tract infection (URTI) was defined as the presence of rhinorrhoea and/or cough in the absence of wheezing, dyspnoea, crackling rales or use of bronchodilator, with or without fever. The classic criteria, presence in an initial episode of acute onset expiratory dyspnoea with previous signs of viral respiratory infection (whether or not this was associated to respiratory distress or pneumonia), were applied in diagnosing bronchiolitis.7 Children with wheezing, breathlessness and obstruction of the airways, in whom similar episodes had previously been diagnosed and treated by a physician, were diagnosed as recurrent wheezing. Cases with focal infiltrates and consolidation in chest radiographs, in the absence of wheezing, were classified as pneumonia.
Only infants born before 28 weeks of GA receive treatment with palivizumab.
Virological studySpecimens of nasopharyngeal aspirates (NPA) were taken from each patient upon admission and sent for virological study at the Respiratory Virus and Influenza Unit (WHO-National Influenza Centre-Madrid, ISCIII, Madrid, Spain). Specimens were processed within 24h of collection. Three RT-nested PCR assays were performed to detect a total of sixteen respiratory viruses. In these assays, reverse transcription (RT) and first amplification round were carried out in a single tube using the Qiagen® OneStep RT-PCR kit (Qiagen, Hilden, Germany). Influenza A, B and C viruses were detected using a previously described method including the primer sets specific to amplify influenza viruses in a multiplex PCR assay.8 From 2003, this assay was used directly in respiratory samples as the routine method for the establishment of primary influenza A, B and C diagnosis at the National Influenza Centre-Madrid. A second multiplex PCR was used to detect parainfluenza viruses 1–4, human coronaviruses 229E and OC43, enteroviruses and rhinoviruses.9 Presence of RSV-A and B types, HMPV, HBoV and adenoviruses were investigated by a third multiplex RT-nested PCR method.10
An internal amplification control was included in the reaction mixture to exclude false-negative results due to specimen inhibitors and/or extraction failure. Given the high sensitivity of nested PCR, precautions had to be taken to prevent reaction tubes from becoming contaminated with previously amplified product as well as to protect target RNA, or DNA, from other specimens and controls. All procedures were performed in safety cabinets located in separated laboratories, all well away from the area where amplified products were analysed. Detection levels of 0.1 and 0.01 TCID50 of influenza A and B viruses and 1–10 molecules of cloned amplified products of influenza C virus, RSV A and B, and adenovirus serotype 1 were achieved.
Statistical analysisIncidence and clinical characteristics of infections in preterm babies were compared with those associated to term infants. Values were expressed as percentages for discrete variables, or as mean and standard deviation for continuous variables. Clinical characteristics and laboratory variables were compared using the Student's t test, the Mann–Whitney U test, the χ2 test, and Fisher's exact test. A two-sided value of p<0.05 was considered statistically significant. All analyses were performed with the Statistical Package for the Social Sciences (SPSS), Version 21.0.
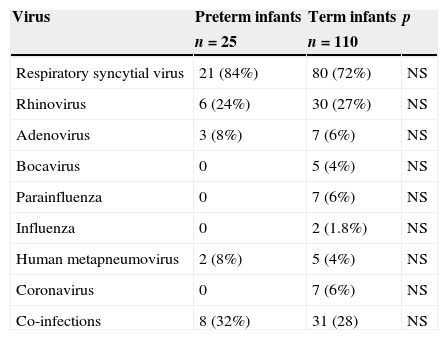
ResultsDuring the study period, 143 preterm infants were born, of whom 30 (20.9%) required admission for respiratory infection, compared with 129 (6.9%) of 1858 term infants born in the same period (p<0.0001, OR 3.6 CI 2.0 to 5.0). The gestational age between the 143 preterm babies was 320–336 (moderate preterm) in 30 cases (21%) and 340–366 (late preterm) in 113 (79%) cases. 33% (10 cases) of the moderate preterm infants required hospitalisation versus 18% (20 cases) of the late preterm babies. A viral agent was identified in 25 of the 30 (83%) episodes in preterm babies, and in 110 of the 129 (85%) of the episodes in term infants. The virus most frequently involved in the preterm infants was RSV (76%) followed by rhinovirus (20%) (Table 1). We detected co-infections in 10% of the cases in moderate preterm babies, in 35% of late preterm infants, and in 25% of those born at term. The most frequent associations were RSV with adenovirus and rhinovirus. We found no differences in the aetiology of infections in preterm and term infants.
Frequency of viruses detected in hospitalised preterm and term infants.
| Virus | Preterm infants | Term infants | p |
|---|---|---|---|
| n=25 | n=110 | ||
| Respiratory syncytial virus | 21 (84%) | 80 (72%) | NS |
| Rhinovirus | 6 (24%) | 30 (27%) | NS |
| Adenovirus | 3 (8%) | 7 (6%) | NS |
| Bocavirus | 0 | 5 (4%) | NS |
| Parainfluenza | 0 | 7 (6%) | NS |
| Influenza | 0 | 2 (1.8%) | NS |
| Human metapneumovirus | 2 (8%) | 5 (4%) | NS |
| Coronavirus | 0 | 7 (6%) | NS |
| Co-infections | 8 (32%) | 31 (28) | NS |
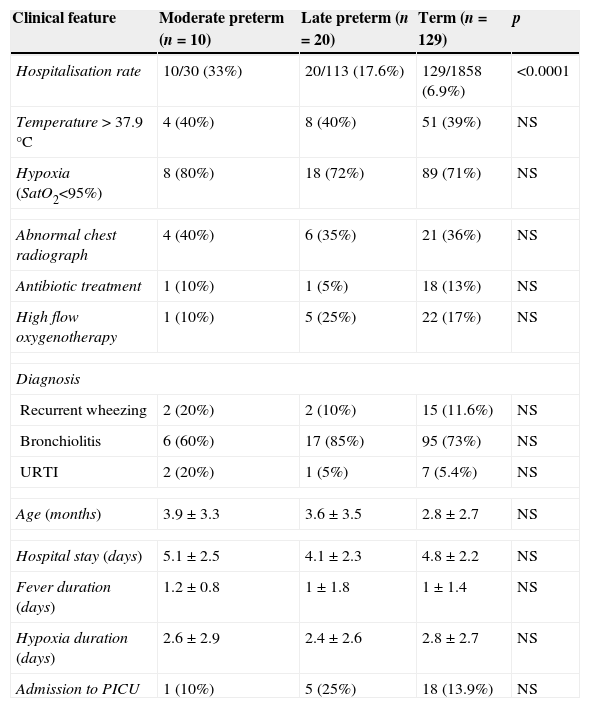
Clinical characteristics of the episodes in the preterm group are described in Table 2. The average age at admission was 5±3.5 months, gestational age at birth 34.4±1.5 weeks, birth weight 2246±469g and male predominance (56%). 68% of those with respiratory infection had a history of having been admitted at birth. Fever was present in 56% and 28% showed pulmonary infiltrates on chest radiography. 68% of them received treatment with epinephrine, 12% with salbutamol and 20% did not receive bronchodilators. 80% of them required oxygen therapy, 24% of them with high-flow system. The average length of hospital stay was 5.43±4.29 days. Four preterm infants required admission to intensive care unit (2.79%), all due to RSV infection. The most frequent diagnosis was bronchiolitis.
Clinical characteristics associated with infections in preterm and term infants.
| Clinical feature | Moderate preterm (n=10) | Late preterm (n=20) | Term (n=129) | p |
|---|---|---|---|---|
| Hospitalisation rate | 10/30 (33%) | 20/113 (17.6%) | 129/1858 (6.9%) | <0.0001 |
| Temperature>37.9°C | 4 (40%) | 8 (40%) | 51 (39%) | NS |
| Hypoxia (SatO2<95%) | 8 (80%) | 18 (72%) | 89 (71%) | NS |
| Abnormal chest radiograph | 4 (40%) | 6 (35%) | 21 (36%) | NS |
| Antibiotic treatment | 1 (10%) | 1 (5%) | 18 (13%) | NS |
| High flow oxygenotherapy | 1 (10%) | 5 (25%) | 22 (17%) | NS |
| Diagnosis | ||||
| Recurrent wheezing | 2 (20%) | 2 (10%) | 15 (11.6%) | NS |
| Bronchiolitis | 6 (60%) | 17 (85%) | 95 (73%) | NS |
| URTI | 2 (20%) | 1 (5%) | 7 (5.4%) | NS |
| Age (months) | 3.9±3.3 | 3.6±3.5 | 2.8±2.7 | NS |
| Hospital stay (days) | 5.1±2.5 | 4.1±2.3 | 4.8±2.2 | NS |
| Fever duration (days) | 1.2±0.8 | 1±1.8 | 1±1.4 | NS |
| Hypoxia duration (days) | 2.6±2.9 | 2.4±2.6 | 2.8±2.7 | NS |
| Admission to PICU | 1 (10%) | 5 (25%) | 18 (13.9%) | NS |
PICU: paediatric intensive care unit, URTI: upper respiratory tract infections.
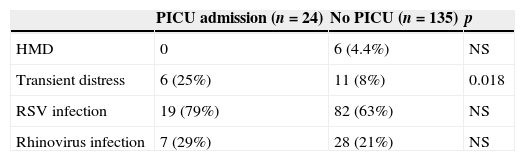
We compared clinical and epidemiological characteristics of episodes among term and preterm infants (Table 2), and we found no statistically significant differences in the parameters studied. 24 patients required admission to intensive care unit, of whom one (10%) was moderate preterm, five (25%) late preterm and 18 (13.9%) were born at term. 25% of them had a personal history of adaptive respiratory distress (p<0.05, OR 2.6 CI 1.238 to 5.827) (Table 3). 66% were younger than a month old on admission to intensive care. None had presented respiratory virus infection during their admission to the neonatal unit. No significant differences were found between the number of moderate and late preterm infants who needed ICU admission.
Clinical characteristics of the patients who require paediatric intensive care (PICU) admission or not.
| PICU admission (n=24) | No PICU (n=135) | p | |
|---|---|---|---|
| HMD | 0 | 6 (4.4%) | NS |
| Transient distress | 6 (25%) | 11 (8%) | 0.018 |
| RSV infection | 19 (79%) | 82 (63%) | NS |
| Rhinovirus infection | 7 (29%) | 28 (21%) | NS |
HMD: hyaline membrane disease.
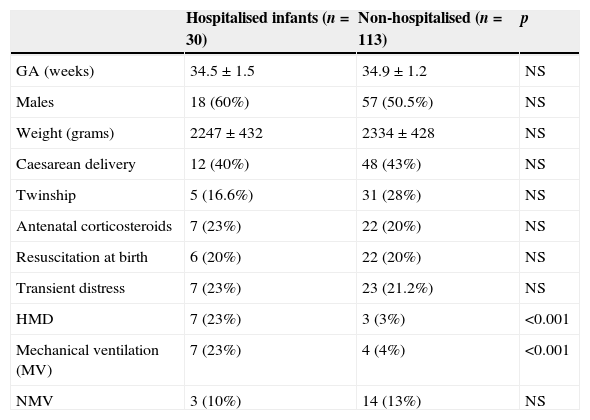
The clinical and demographic characteristics of the group of preterm infants who required hospitalisation (n=30) are shown in Table 4 and compared with the other preterm infants (n=113). There was no difference in mean gestational age at birth; sex; weight; being born by caesarean section; being twins; having received antenatal steroids or having suffered adaptive respiratory distress at birth. Children required admission presented more frequently hyaline membrane disease (HMD) at birth (p<0.001, OR 7.7 CI: 2.121 to 27.954) and needed mechanical ventilation (p<0.001, OR 5.7 CI: 1.813 to 18.396).
Epidemiological and clinical characteristics during neonatal period of the preterm infants who require hospitalisation or not.
| Hospitalised infants (n=30) | Non-hospitalised (n=113) | p | |
|---|---|---|---|
| GA (weeks) | 34.5±1.5 | 34.9±1.2 | NS |
| Males | 18 (60%) | 57 (50.5%) | NS |
| Weight (grams) | 2247±432 | 2334±428 | NS |
| Caesarean delivery | 12 (40%) | 48 (43%) | NS |
| Twinship | 5 (16.6%) | 31 (28%) | NS |
| Antenatal corticosteroids | 7 (23%) | 22 (20%) | NS |
| Resuscitation at birth | 6 (20%) | 22 (20%) | NS |
| Transient distress | 7 (23%) | 23 (21.2%) | NS |
| HMD | 7 (23%) | 3 (3%) | <0.001 |
| Mechanical ventilation (MV) | 7 (23%) | 4 (4%) | <0.001 |
| NMV | 3 (10%) | 14 (13%) | NS |
GA: gestational age, HMD: hyaline membrane disease, NMV: non-invasive mechanical ventilation.
We present a cohort of preterm and term infants which has been studied prospectively. Respiratory viral infections of enough severity to require admission have been analysed, and a complete panel of viruses has been detected. In our series, preterm infants between 320 and 366 weeks have a higher incidence of admission because of respiratory viral tract infections than term infants. When they were compared with term infants, moderate and late preterm infants have 3.6 times higher risk of requiring admission for respiratory infection during the first year of life (p<0.001). This risk is further increased if during the neonatal period they presented hyaline membrane disease and/or needed invasive mechanical ventilation (p<0.001). Nevertheless, once admitted, the clinical features of respiratory infection episodes requiring hospitalisation are similar among those born at term and preterm. Severity indicators are similar, included the need for intensive care unit admission.
Taken together, the results of the published studies suggest that birth between 320 and 366 weeks GA is a very important risk factor for respiratory morbidity during infancy and early childhood. The physiological deficiencies that result from incomplete lung development are likely to account for the early morbidity and vulnerability to infection.11 A modest but growing body of literature has documented the broad range of complications that late-preterm infants may experience. Colin et al.11 in a review of the literature, found 24 studies, 16 of which were retrospective population-based cohort studies; and eight were observational, most of which focused on RSV infection. They found that infants born at 32–36 weeks GA, experience substantial respiratory morbidity compared with term infants. Respiratory distress syndrome at birth has been described as a risk factor for hospitalisation in the first year of life.4 Also, in our patients, infants with HMD and needing mechanical ventilation were more frequently hospitalised and probably are the group which needs most attention.
There are different studies about the severity of RSV infections in preterm infants. Horn and Smout12 found that infants between 32 and 35 weeks GA, had a higher risk of severe outcomes than term infants, because they needed more frequent intensive care admission and mechanical ventilation. In our experience, with the limitation of the small number of preterm infants, we did not find any differences in the frequency of PICU admission in preterm and term infants. Clinical characteristics of the episodes in hospitalised infants were similar for preterm and term infants.
Although RSV infections have been frequently studied, we have found only limited information about other viruses and preterm infants. In our series, rhinovirus is the second virus associated with respiratory viral infections in this group of patients. Additionally, we have seen no differences in severity of infections or need for intensive care unit admission, neither between preterm and term infants nor between RSV and rhinoviruses. Miller et al.13, in Argentina, found that HRV is the most frequent agent identified in very low birth weight during the first year of life, and it is also more frequently responsible for hospitalisations than RSV. Bronchopulmonary dysplasia and absence of breast feeding were risk factors for hospitalisation. These patients did not receive palivizumab.
Finally, we think that rhinoviruses are as important as RSV, and special attention must be paid in this group of patients. Nevertheless, the number of preterm infants in our series is small, and large prospective studies including all the respiratory viruses are necessary to clarify the role of the other viruses in hospitalisations of preterm infants in early infancy.
Ethical disclosuresPatients’ data protectionConfidentiality of data. The authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
Protection of human subjects and animals in researchThe authors declare that no experiments were performed on humans or animals for this investigation.
FundingThis work was partially supported by ISCIII, Fondo de Investigaciones Sanitarias grant PI 09/00246, PI12/012.
Conflict of interestThe authors declare no conflict of interest.
