






Exposure to house dust mites (HDMs) is a major risk factor for the development of allergic symptoms. HDMs are worldwide in distribution. Assessing these allergens in each area is a critical step in evaluating the risk of sensitisation and controlling allergic symptoms. The aim of the present study was to evaluate the level of major HDMs, Der p 1 and Der f 1, in various parts of Iran.
MethodsIn 2009, 257 dust samples were obtained from living rooms’ carpets in seven cities throughout Iran with different geoclimatic conditions. The level of Der p 1 and Der f 1 was measured by commercial ELISA.
ResultsDetectable level of Der p 1 and Der f 1 levels were only found in Gorgan and Sari, two cities near the Caspian Sea with moderate temperatures and high relative humidity. In both of these cities, Der f 1 was more frequent than Der p 1 (100% vs. 85%) and was found to be at a higher level than Der p 1 (geometric mean 3128 vs. 439ng/g dust, P<0.001).
ConclusionThe results of this study confirm that house dust mites in Iran are restricted to the Caspian Sea coastal areas, and in other parts, due to seasonal variations of temperature and humidity mites are not able to grow well and therefore are not an important risk factor for sensitisation and respiratory allergies.
Allergic disorders are among the major health problems in the world and many epidemiological studies have reported a dramatic increase in prevalence of asthma and other allergic diseases over recent decades.1–3 The fact that the prevalence of allergic disorders has been increasing reveals the role of many factors, but exposure to allergens is the most important risk factor for development of allergic diseases.4–7
Among aeroallergens, indoor allergens have a great role in allergic sensitisation because these days most people spend considerable amounts of time indoors, especially at home and several studies have shown that sensitisation to indoor allergens correlates well with indoor allergen exposure.8–13
A large proportion of asthmatic and allergic patients is sensitised to indoor allergens, especially house dust allergens such as house dust mite, animal dander, cockroach and moulds. Among them, house dust mite (HDM) allergens are very important and their role in the sensitisation and development of allergic symptoms, particularly in asthma and rhinitis, has been documented in many studies around the world.14–18 It has been reported that between 60 and 100% of asthmatic subjects have hypersensitivity to house dust mite allergens.19
Mites are members of the spider family belong to Arachnids, and at least 50 species of mites have been detected in dust.20 Among them, the house dust mites, Pyroglyphidae family, including Dermatophagoides pteronyssinus and Dermatophagoides farinae, are the most important in terms of allergenicity and clinical relevance.21,22 They have two major allergens, Der p 1 and Der f 1, which elicit IgE antibody responses in the majority of patients who are sensitive to pyroglyphid mites.22
Identification of the most prevalent allergens in each area has a very important role in the prevention, diagnosis and treatment of allergic disorders. Moreover, information about the most important aeroallergens in each area has significant impacts on both the diagnosis as well as the treatment of allergy.
HDMs are common throughout the world, but as their growth depends on geoclimatic factors, a great variation in the level of HDMs was seen in different regions.23 Iran is a fairly large country with different geoclimatic conditions particularly regarding temperature, humidity and altitude, ranging from arid or semiarid in the central parts to humid subtropical ones alongside the Caspian Sea in the north and the Persian Gulf in the south. In spite of the important role of HDM allergens in asthma and other allergic diseases, there are no data about the presence and level of HDM allergens in different regions of Iran except for one old report.17,24–27
The purpose of the present study was to determine the abundance of two important HDM allergens, Der p 1 and Der f 1, at homes in seven cities with different geoclimatic conditions throughout Iran.
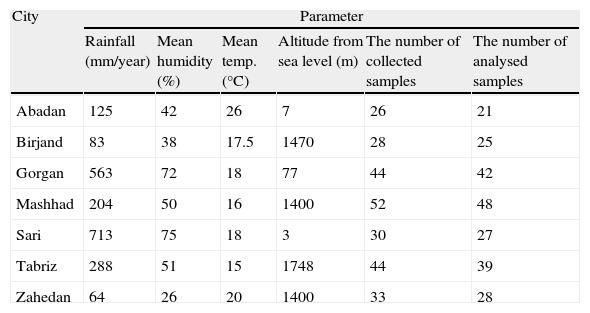
MethodsHouse dust samplingFrom August to October 2009, a total of 257 samples were collected from living rooms’ carpets in seven cities: Abadan, Birjand, Gorgan, Mashhad, Sari, Tabriz, and Zahedan which are located in different parts of Iran with different geoclimatic conditions. Fig. 1 and Table 1 show the location map and geoclimatic parameters of all the cities, adopted from the Islamic Republic of Iran Meteorological Organization (www.irimet.net).

Geoclimatic parameters of the cities, where house dust sampling was done throughout a Persian year (20/3/2009 to 20/3/2010).
| City | Parameter | |||||
| Rainfall (mm/year) | Mean humidity (%) | Mean temp. (°C) | Altitude from sea level (m) | The number of collected samples | The number of analysed samples | |
| Abadan | 125 | 42 | 26 | 7 | 26 | 21 |
| Birjand | 83 | 38 | 17.5 | 1470 | 28 | 25 |
| Gorgan | 563 | 72 | 18 | 77 | 44 | 42 |
| Mashhad | 204 | 50 | 16 | 1400 | 52 | 48 |
| Sari | 713 | 75 | 18 | 3 | 30 | 27 |
| Tabriz | 288 | 51 | 15 | 1748 | 44 | 39 |
| Zahedan | 64 | 26 | 20 | 1400 | 33 | 28 |
In each city, houses were selected based on random telephone number sampling by a computer program procedure. Briefly, one square metre of a living rooms’ carpet, vacuumed for 2min with a 1200-W vacuum cleaner equipped with a dust collector and filter (Indoor Biotechnologies, Charlottesville, VA, USA). All carpets had not been cleaned for at least five days prior to the sampling and the samples were picked from an area far from direct sun light. After vacuuming, the filter was removed and kept in zip-lock plastic bags at 4°C to prevent the growth of mites. Due to the low amount of the dust sample, 27 samples were excluded and processing was done on the 230 remaining samples.
Extraction of HDM allergensBefore extraction, dust samples were sieved through a 345μm mesh and fine dust was weighed. Then 2.0ml PBS–T (0.05% Tween 20 in phosphate buffered saline, pH 7.4) was added to 100mg of fine dust. For samples between 20 and 100mg, a proportional amount of buffer was added. Samples less than 20mg were excluded and not processed. After 2h mixing on rocker at room temperature, samples were centrifuged for 20min at 2500rpm at 4°C and the supernatant was removed carefully and kept at −20°C until analysis.
Enzyme linked immunosorbent assay (ELISA)Levels of Der f 1 and Der p 1 were measured using commercial ELISA kits (Indoor Biotechnologies, Charlottesville, VA, USA) as described in the manufacturer's instructions. All samples were tested in duplicate and the average value was considered. The levels of Der f 1 and Der p 1 were expressed as ng/ml or ng/g of dust. The lower detection limit for both kits was 0.5ng/ml or 10ng/g dust.
Statistical analysisData were analysed using SPSS, version 16.0 (SPSS Inc., Chicago, IL, USA). Since the allergen concentrations in Gorgan and Sari followed a non-Gaussian distribution, calculations were carried out on log-transformed data. Geometric means (GM) with 95% confidence interval (CI) were obtained for the allergen levels. The differences between the means were analysed by the Mann–Whitney test. The correlation between allergens was carried out by the Spearman's non-parametric correlation test.
ResultsAmong 230 processed and tested samples, 59 samples (26%) were found positive (higher than 0.5ng/ml or 10ng/g of dust sample) for both Der f 1 and Der p 1. Interestingly, all positive samples had been collected only from Sari and Gorgan, two cities located in the coastal area of the Caspian Sea with high humidity and moderate temperatures. Samples from all other cities were negative for both Der p 1 and Der f 1 (Fig. 2a and b).
 and Der f 1 (b) allergens in house dust samples from Gorgan and Sari. The horizontal bars indicate the geometric means (GM).")
In both cities, Sari and Gorgan, all samples were positive for Der f 1 but only 86% and 85% of samples were positive for Der p 1 in Gorgan and Sari, respectively. Der f 1 was also found at a higher level than Der p 1 (geometric mean 3128 vs. 439ng/g dust, P<0.001) in positive samples (Fig. 2b).
In 70% of positive samples, the level of Der f 1 was higher than 2000ng/g dust which is considered as the threshold of sensitisation, but this percentage was 16% for Der p 1 (Fig. 3a and b).
 and Sari (b). Dashed line is sensitisation threshold of 2000ng/g.")
In positive samples from Gorgan, there was a weak but significant correlation between the level of Der p 1 and Der f 1 (Spearman's R=0.382, P<0.05) while in Sari, correlation between the level of Der p 1 and Der f 1 was not significant (Spearman's R=−0.167) (Fig. 4a and b).
Discussion and Sari (b).")
Exposure to HDM allergens is a major risk factor for the sensitisation and development of asthma and allergic diseases28 but the level of allergens is quite variable in different regions. HDM populations and the amount of allergens are influenced by many factors, especially geoclimatic parameters. Considering the importance of HDM in the sensitisation and development of allergic diseases and the lack of enough information about the level of mites in different regions of Iran, the present study was conducted.
It has been proven that carpets at homes are the main source of HDM.29 In Iran, due to cultural habits, carpets have a great contribution and value to people's life. The carpets are usually stretched from wall-to-wall in Persian houses. For these reasons, we collected dust from living rooms carpets as the main source of allergens.
In this study, mite allergens were only found in Sari and Gorgan, two cities near the Caspian Sea. Previous studies had shown that optimum condition for mite growth were the temperature ranging between 20 and 30°C and relative humidity higher than 60%.30
Based on the meteorological data in the two years, 2009 and 2010, the number of days which had optimum conditions for mites growth, was accounted 0, 0, 1, 1, 12, 134 and 151 days in Birjand, Zahedan, Mashhad, Tabriz, Abadan, Gorgan, and Sari, respectively. Thus, only Gorgan and Sari had enough days with optimal conditions.
These results are concurrent with two previous studies in Iran. In Amoli's study, mites were found only in the Caspian Sea region24 and Soleimani et al. reported the presence of mites in hotels and inns in Bandar-Abbas, a port located in the Persian Gulf with a warm and humid climate.31 It should be mentioned that mite allergens were also detected in hot and dry regions, like Kuwait and Sistan and Baluchestan province of Iran17,32 and this is possibly because of a wide use of air conditioners in the houses which make indoor air suitable for the growth of mites.
Some studies about the most common aeroallergens among allergic patients in several cities of Iran including Shiraz,25 Mashhad,26 Karaj27 and Birjand (Fereidouni M, unpublished data) confirm our finding too. In all those cities, the prevalence of sensitisation to HDM allergens was reported to be around 20% in allergic rhinitis patients, which is considerably lower than sensitisation to other aeroallergens such as pollen in the same cities. In contrast, in humid areas like Sari in the north of Iran,33 Thailand, and Malaysia18,25,34,35 the rate of sensitisation to mite allergens is high as all those four cities have fairly dry climates, lack of mite infestation may be the reason for the low rate of sensitisation to mite allergens.36
It is worth mentioning that the presence of sensitisation to HDM despite the inability of mites to grow in dry climates could be explained by cross reactivity between different allergens or previous exposure to HDM allergens in a different time period throughout their life.
Among the positive samples, Der f 1 was more prevalent and had a higher level than Der p 1, while in previous studies from coastal areas in the north and south of Iran, direct microscopic examination identified D. pteronyssinus more frequently.24,31 This discordance could be clarified by difference in study methodology or by considering that winter in Sari and Gorgan is cold and D. farinae is more resistant to climate variation than D. pteronyssinus.37,38
In conclusion, this is the first nationwide study which confirms that house dust mites in Iran are restricted to a small area close to the Caspian Sea. While, in other parts, due to seasonal variations of temperature and humidity; mites are not able to grow well and therefore are not important risk factor for sensitisation and respiratory allergies.
Ethical responsibilitiesProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
FundingThis study was made possible by a grant from the Research Vice Presidency of Birjand University of Medical Sciences.
Conflict of interestThe authors have no conflict of interest to declare.
This study was made possible by a grant from the Research Vice Presidency of Birjand University of Medical Sciences (BUMS). We thank all study participants for their kind cooperation.
