



Primary immunodeficiencies (PID) are genetic diseases that affect the immune system and for the last 20 years, the Latin American Society for Immunodeficiencies (LASID) has been promoting initiatives in awareness, research, diagnosis, and treatment for the affected patients in Latin America. These initiatives have resulted in the development of programmes such as the LASID Registry (with 4900 patients registered as of January 2014), fellowships in basic and clinical research, PID summer schools, biannual meetings, and scientific reports, amongst others. These achievements highlight the critical role that LASID plays as a scientific organisation in promoting science, research and education in this field in Latin America. However, challenges remain in some of these areas and the Society must envision additional strategies to tackle them for the benefit of the patients. In June 2013, a group of experts in the field met to discuss the contributions of LASID to the initiatives of PID in Latin America, and this article summarises the current state and future perspectives of this society and its role in the advance of PIDs in Latin America.
Primary immunodeficiencies (PID) are inborn errors of immunity that affect the production of cells and/or molecules leading to abnormalities in the ontogeny, differentiation or effector function of the immune system. According to the latest report in 2011 of the Experts Committee on Primary Immunodeficiency of the International Union of Immunological Societies (IUIS), more than 160 genetic defects lead to a wide spectrum of PID in humans, with variable clinical impact on the immune function as well as in other systems.1 However, with the advances in genomics and bioinformatics, this number is estimated to grow to more than 230 genetic defects within one year, including an expanding number of phenocopies that result from autoantibodies and other mechanisms that affect immune function. PID manifests more often early in life and commonly as high susceptibility to infections with a clinical spectrum that ranges from single episodes of severe and life-threatening infections, to recurrent and chronic infections and caused by a myriad of microorganisms. However, PID can also manifest predominantly or in a combination with other abnormalities such as autoimmunity, autoinflammation, haemophagocytosis, allergies and higher susceptibility to certain forms of cancer, amongst others.2 The actual prevalence of PID in the general population is unknown but based on estimates from published cohorts of patients in different countries, it has been suggested to be about 1/10,000 in the general population, however, recent reports support the postulate that they are more common than previously estimated.3,4
Despite a considerable increase in the knowledge about PID, diagnosis and treatment remain a problem. More specifically, countries in Latin American frequently face challenges related to human, economic and scientific resources, access to technology and government policies. This article introduces the Latin American Society for Immunodeficiencies (LASID) and describes how this society has been working in recent years, to provide solutions to the challenges that immunologists and patients encounter in this part of the world.
From The Latin American Group of Primary Immunodeficiencies (LAGID) to the Latin American Society for Primary Immunodeficiencies (LASID)In the late eighties, a group of physicians from several Latin American countries became interested in promoting awareness and scientific and clinical knowledge about immunology and the diseases of the immune system in their continent. By April 1993 and during the meeting of the Latin American Association of Immunology (Asociación Latinoamericana de Inmunología, ALAI) that took place in Santiago (Chile), this group of doctors from Argentina, Brazil, Chile and Colombia created the Latin American Group for Immunodeficiencies (LAGID). They set the goals of creating a registry of patients with PID to learn more about the state of these diseases in this part of the world, and to optimise diagnostic and therapeutic resources and develop collaborative research projects.
As part of the first efforts towards a registry, the LAGID group published the first two epidemiological reports on PID in Latin America in 1998 and 2007, respectively.5,6 The first report included 1428 patients from eight countries (Argentina, Brazil, Chile, Colombia, Costa Rica, Mexico, Paraguay, and Uruguay), comprising antibody deficiencies in 58% of patients, combined immunodeficiencies in 23%, phagocytic disorders in 17%, and complement deficiencies in 2% of patients. In the second report in 2007, the number of patients rose to 3321 cases from 12 countries (Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Ecuador, Mexico, Peru, Paraguay, Uruguay, and Venezuela), with similar distribution of groups of diseases as reported previously. In fact, all the countries involved in the first publication reported an increase of cases in the second one, illustrating ongoing efforts to improve PID diagnosis in Latin America.
Education in PID at LASIDSince its inception as LAGID and as one of the main goals of LASID, its members have been hosting scientific meetings with experts from all over the world, to promote interactions amongst physicians and researchers from the Latin America. Twelve annual meetings were conducted in Chile, Argentina, Brazil, Mexico, Colombia, Uruguay, and Costa Rica from 1993 to 2007. Then in 2009, when LAGID became the Latin American Society for Primary Immunodeficiencies (LASID), its members held their first meeting as a Society in Cartagena de Indias (Colombia); then the second one in 2011 at Mexico City (Mexico) and the third meeting in October 2013 in Santiago (Chile). These biannual meetings are intended not only for immunologists, but also for general physicians and specialists such as paediatricians, haematologists, infectious diseases specialists, and rheumatologists, amongst others. These biannual meetings also include a concurrent meeting of local and regional patients associations. Support for these meetings has been provided by National and International Scientific and Medical Organizations such as the National Associations of Allergy, Asthma and Immunology, Pediatrics, etc., as well as the European Society for Immunodeficiencies (ESID) and the Clinical Immunology Society (CIS), to name a few. Additional funding has come from local government agencies such as The Administrative Department of Science, Innovation and Technology (Colciencias) in Colombia, Fundação de Amparo a Pesquisa do Estado de São Paulo (Fapesp) and Conselho Nacional de Desenvolvimento Cientifico e Tecnológico (CNPq) in Brazil, and The National Council of Science and Technology (Conacyt) in Mexico. One of the most significant sources of funding has been the Jeffrey Modell Foundation (JMF) that not only provides resources for the Jeffrey Modell Diagnostic and Research Centers throughout the continent, but also for specific projects such as the LASID Registry. Other important patient organisations have also provided support including the International Patient Organization for Primary Immunodeficiencies (IPOPI) and the RAGIS society.
One of the fundamental interests in our society has been to evaluate the situation of PID in most countries of Latin America from several perspectives, in order to focus the Society's efforts towards providing possible solutions to its existing problems. These assessments led by experts in Advisory boards and surveys conducted with its members, have been followed by several publications that present an in-depth analysis of the different circumstances and situations that impact PID throughout the region, and the potential solutions to overcome them. The first paper of this series entitled “Primary Immunodeficiencies in Latin America” discussed critical issues and needs in the diagnosis and management of these diseases in our region.7 Three more papers have been produced since then, focusing on the implementation of strategies in education and registry, training and development of laboratory networks, trying to provide possible solutions.8–10 However lately, members of these boards in the Society have been focusing on publications that are more oriented to providing tools for diagnosis, as well as the treatment of PID such as the recent guidelines for the use of IVIg in PID in Latin America, respectively.11,12
LASID has also held biannual Summer Schools in PID as part of its educational programme since 2006. The structures of the courses are similar to those of CIS and ESID. Each school hosts an average of 30 young fellows that interact permanently with a selected group of faculty experts in the field. The course includes the presentation of reviews in selected topics, real clinical cases and research projects by the applicants with the guide of experts, and open discussions and forums.
Research at LASIDOne of the most important initiatives of LASID has been the development of the Online Registry (http://imunodeficiencia.unicamp.br:8080/estatistica_mensal.html). It is a platform based on the ESID Registry and it was officially launched in 2009 with the participation of 25 registering centres from seven countries. The JMF, the National Council for Scientific and Technological Development from Brazil (Conselho Nacional de Desenvolvimento Científico e Tecnológico, CNPq), Baxter Bioscience and the State University of Campinas, provided the funding this initiative. Currently, support comes from the CNPq, the JMF, Baxter Bioscience, Octapharma, and CSL Behring.
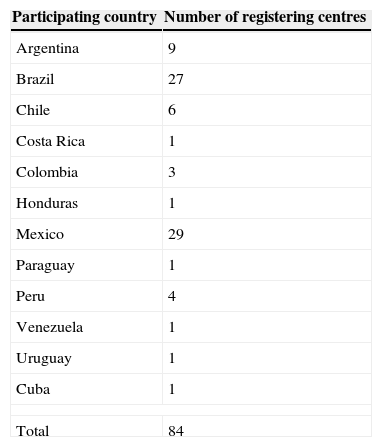
The LASID Registry collects basic information about the diseases affecting patients in every participating country. Specific information regarding the clinical and laboratory presentation of most PID is entered by the participating centres, and basic statistics are generated about every two months containing not only the number of patients and their diseases, but also the degree of input from every centre registering the patients. The core of the Registry is to serve as a platform that will foster clinical research on the different aspects of PID such as epidemiology, the genetic basis of these diseases, diagnosis and treatments, amongst others. In addition, the Registry collects information about the use of immunoglobulin replacement therapy for the different diseases. All this information is freely available on the Registry's website; however, access to the registration of patients is granted only to Medical Institutions, Universities and Research Centres that meet the local IRB requirements to become Registering Centres. As of January 2014, 87 institutions from 13 countries are officially part of the Registry (Table 1).
Registration of patients involves the collection of demographic variables as well as the most prevailing signs and symptoms leading to the phenotypic diagnosis, as well as the molecular definition of the disease whenever is possible. As of January 2014, there are 4900 cases in the Registry with Argentina being the country with the highest number of patients registered: 1869 patients (38.14%), followed by Brazil with 1095 patients (22.35%), Colombia with 781 cases (16.94%), and Mexico with 754 cases (15.39%). Based on estimates of the global prevalence of PID and the current population of 600 million people in Latin America, we think that the number of patients could be approximately in the vicinity of 58,000 patients. Therefore, the current number of registered cases represents only a fraction of the potential number of patients that can be found and incorporated into this database. By grouping the patients according to the IUIS groups of PID, their current frequency in the LASID registry is: predominantly antibody deficiencies representing 52% of the cases, followed by well-defined immunodeficiency syndromes (19%), combined immunodeficiencies and defects in phagocyte number, function or both (9% each), autoinflammatory disorders (6.2%), complement deficiencies (2.5%), defects in innate immunity (1.3%) and diseases of immune dysregulation (1%) (Figure 1). Interestingly, when the Registry is sorted by country, one notes that some diseases seem to be more prevalent in certain areas than others. For example, more patients with ataxia telangiectasia have been registered in Mexico and Costa Rica, suggesting that this disease might be more prevalent in Central America. It will be very important to validate this and other information with larger sets of data, to actually determine if the higher frequency of some phenotypes/region, might be the result of founder effects 13 or alternatively, the effect of some skewing by active local registries.

Phenotypic distribution by percentages of all PID in the LASID registry according to the classification of the IUIS Expert Committee on PID.1
Registries can also be used to figure out the effectiveness of the educational initiatives leading to better diagnosis and treatment of PID. Our preliminary analysis of the data entered by the different participating centres is showing regional differences in terms of the rate of registration, the quality of the information entered into the databases, the use of diagnostic tools, and even the differences in the modalities of treatments administered to the patients. As a result of this, the training sessions have been readdressed to emphasise the importance of the accuracy of the data before it is entered into the database, so the sets of information are homogeneous in order to generate reliable information.
Finally, the Registry is also allowing us to learn about unusual phenotypes associated to known genetic defects, as well as to decipher novel molecular genetic defects and the molecular basis of these in patients in Latin America. Members of LASID are currently conducting three multicentre clinical and epidemiological studies on Chronic Granulomatous Disease (CGD), CD40L Deficiency (formerly X-linked Hyper-IgM syndrome or X-HIGM), and Agammaglobulinaemia. Specifically, preliminary results of the CGD study are revealing a high incidence of BCG vaccine adverse reactions in these patients, reaching approximately 20% of cases. In the Agammaglobulinaemia study the results are pointing out a significant delay in the diagnosis as well as complications related to it such as vaccine-derived poliovirus infections, and a series of lung sequelae due to recurrent pulmonary infections. Finally, in the CD40L Deficiency study, the results are showing that most patients have a very high rate (up to 85%) of severe fungal infections (Condino A, et al., manuscript in preparation). Most patients along with the clinical and laboratory information related to the diagnosis and treatment were obtained through the LASID Registry, demonstrating its power as a tool that also contributes to better define PID in the patients and Latin America. These results are helping us to focus on the commonalities as well as the uniqueness of these, and the kind of strategies that LASID must implement to promote better diagnosis and treatment.
Research with the use of the LASID Registry represents one initiative that provides interaction and fosters collaborations in our countries. However, it is only a fraction of the basic and clinical research performed by many groups in Latin America (alone or in collaboration with institutions throughout the world) in recent years. These have led to many peer-reviewed publications related to the description of new phenotypes and case reports, the immunological and molecular basis of known and novel PID, and novel strategies for the treatment of these diseases, among others.
Diagnosis of PID in Latin AmericaLatin America is not new to the world of PID. The creation of LAGID 20 years ago brought new possibilities for the diagnosis and treatment of patients in our region. Working groups were created in Argentina, Brazil, Mexico, Colombia, Chile, Costa Rica, and many more. Practically all these groups have grown to become public or private reference centres in their own countries, providing not only access to diagnosis and treatment but also generating knowledge with cutting-edge research, creating undergraduate and graduate programmes in basic and clinical immunology and PID, and generating a number of internationally recognised educational initiatives in some cases, with the help of local Patient Organisations.
These achievements have called the attention of international organisations such as The JMF, ESID, IPOPI and the Clinical Immunology Society (CIS), who have joined LASID in their effort to improve research, diagnosis and treatment of patients in Latin America. The JMF for example, started by incorporating physicians from most of the centres in our Region into their network of referring physicians and since 2007, has been establishing Jeffrey Modell Diagnostic and Research Centers throughout the region (Sao Paulo, Brazil), Mexico City (Mexico), Medellin (Colombia), Buenos Aires (Argentina) and Santiago and Temuco as a Network (Chile). Additional JM networks are being planned in other countries. They have also provided a number of small grants to local patient organisations to promote education and awareness in their communities of patients. IPOPI has also been working with LASID and the patient organisations throughout the region to improve access to diagnosis and treatment. ESID and CIS have also teamed up with LASID to create a partnership that is providing shared membership to all three societies with full benefits to all their members. These benefits include access to publications, registries and training in PID, as well as grants and support for educational initiatives.
A number of groups throughout the region are now able to provide specialised tests for more accurate immunological and molecular diagnosis such as in Argentina, Brazil, Mexico, Colombia, Uruguay, Costa Rica and Chile, among others. These and other initiatives have the support of public agencies and private organisations (both locally and internationally).
Treatment of patients with PID in Latin AmericaThe treatment of patients with PID might vary depending on the underlying defect. However, providing an integral treatment dealing not only with the immune therapy but also with the support, requires understanding in order to actually impact the quality of life of the patients. Considerations must be placed at providing proper nutrition and diet when required, respiratory therapy, prophylactic antimicrobials and psychological support. Most PID affecting the production of antibodies might at some point require the supplementation of antibodies in the form of gammaglobulin. Other types of therapies might include replacement with recombinant cytokines, enzymes, etc. Finally, specific immunological intervention might require Haematopoietic Stem Cell Transplantation (HSCT) and even Gene Therapy in selected cases.
One of the main concerns regarding PID is the availability of some of these treatments. Intravenous gammaglobulin (IVIg) is available in most countries in Latin America but subcutaneous immunoglobulin (SCIg) is currently available only in a handful of these, and treatments are usually provided by government agencies or private insurance companies. HSCT is only available in available in Brazil, Mexico, Chile, Argentina and Colombia, where there are expert teams on this field. However the framework for this therapy relies not only on the transplantation teams but also in the availability of donors from private institutions or from cord blood banks; and these options vary widely depending on every country. Clearly, this is one of the areas in which LASID is placing significant efforts to provide sources of training and alternatives where those units are insufficient, due to the increasing number of PID patients requiring permanent reconstitution of their immune system. Members of LASID have been working to provide guidelines for treatment of PID and the most recent publication was devoted to the use of IVIg in PID in Latin America.11 However, as the different Centres move towards more refined therapies, LASID must work to insure that guidelines for the use of SCIg and other replacement therapies are worked out properly.
Twenty years ago, a dream became true with the creation of an interest Group that set the basis of what LASID is today. There are many challenges ahead, but the consolidation of this Society is already insured with the input of its clinicians and scientists as well as the incoming generations of young researchers and physicians that make up this organisation.
Conflict of interestThe authors have no conflict of interest to declare.
Ethical disclosuresConfidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Protection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
The authors thank Kedrion Pharma for providing support for this advisory board and for the editorial assistance.
