




Angiotensin-converting enzyme (ACE) gene I/D polymorphism might be linked to the risk of the allergic rhinitis (AR).
ObjectiveIn the present study, we assessed the association of ACE gene I/D polymorphisms with AR susceptibility using a meta-analysis.
Materials and methodsWe carried out a retrieval of studies and included the eligible studies if they met the criteria. After the data extraction, the Stata software was used to analyse the genotype frequencies.
ResultsIn total, five studies with 561 patients and 603 controls were included. However, the genotype distribution among the control of one study was not consistent with the Hardy–Weinberg equilibrium. After pooling all studies, the results indicated an association between ACE gene I/D polymorphism and AR risk in the overall analysis (II vs. others: OR=0.70, 95% CI=0.54–0.92, P=0.010; D vs. I: OR=1.29, 95% CI=1.08–1.54, P=0.005). In the further analysis of the East Asians, no association between ACE gene I/D polymorphism and AR risk was observed.
ConclusionACE gene I/D polymorphisms were not associated with the risk of AR in East Asians. These results need to be confirmed in the following studies.
Angiotensin-converting enzyme (ACE) is a zinc metallopeptidase which is widely distributed on the surface of endothelial cells in all body tissues and secreted in a soluble form in plasma.1 It is known that ACE plays an essential role in the production of angiotensin II and the degradation of bradykinin. So ACE is well known to be a key regulatory factor of the cardiovascular activity and inflammatory response. Further studies showed that plasma ACE activity level was affected by the presence (insertion, I) or absence (deletion, D) sequence of the ACE gene which was located on chromosome 17. As a result, the variation in ACE gene I/D polymorphisms may induce the development of some diseases. Previous studies have shown that ACE gene I/D polymorphisms were associated with the risk of type 2 diabetes, hypertension and psoriasis.2–4
Atopy is an inherited disorder characterised by the tendency to induce immediate allergic reactions after exposure to allergens such as pollen, mites, and insect venoms. Although allergic asthma and allergic rhinitis (AR) have been considered to be a single disease, in some cases they were two common types of atopic disease.5 Several studies have shown the I/D polymorphism of ACE gene to be implicated in susceptibility to asthma,6 and Hollá et al. also investigated that the I/D polymorphism might be linked to the risk of the AR7; however results in other studies have been controversial.8–12 Therefore in the present study, we assessed the association of ACE gene I/D polymorphisms with AR susceptibility using a meta-analysis.
Materials and methodsLiterature search strategyStudies were identified through PubMed, the Cochrane Library and Chinese databases such as the China National Knowledge Infrastructure (CNKI) using the search terms: angiotensin-converting enzyme OR ACE, polymorphism(s) OR allele(s), variation OR genotype(s) AND allergic rhinitis. All studies were limited to human subjects and with no language restriction. In order to obtain adequate studies, two investigators further searched and analysed the references listed in retrieved original and review articles.
Selection criteriaWe included the eligible studies in this study as they met the following criteria: (1) Case–control study; (2) It assessed the association between ACE gene I/D polymorphisms and the susceptibility to AR; (3) The study involved in the frequencies of one or more of the alleles, such as I or D in cases and controls; and (4) Frequencies of ACE gene I/D polymorphism in the controls must be in the Hardy–Weinberg equilibrium (HWE).
Data extractionThe titles and abstracts of retrieved documents were independently screened by two investigators. Studies were excluded if they failed to meet the above-mentioned criteria. Only the latest article was included when there were duplicated articles. The full texts for the included articles were obtained and further evaluated.
We extracted the following information from each included study: the first author, year of publication, country, ethnicity, total numbers of cases and controls, genotypes and alleles frequencies of ACE gene.
Statistical analysisThe associations between ACE gene I/D polymorphism and AR were assessed by calculating the pooled odds ratios (ORs) and corresponding 95% confidence intervals (95% CIs). The heterogeneity among those studies was evaluated using the Cochrane Q-test. I-square was used to quantify the size of heterogeneity. If I-square <30%, it means that there was no obvious heterogeneity among the included studies, and the data were pooled using the fixed-effects model. However, if I-square >30%, there was obvious heterogeneity and thus we selected the random-effects model. The potential publication bias was tested with the funnel plot and Egger's test. We analysed the data using Stata software (version 11.0; Stata Corp., College Station, TX, USA).
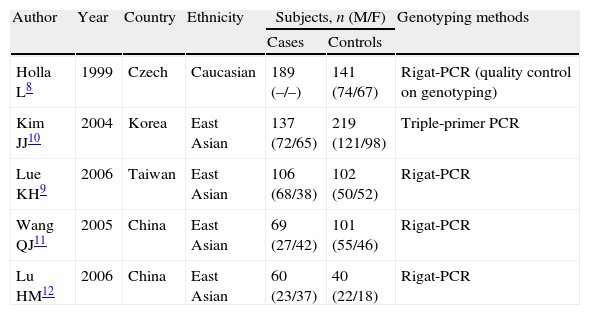
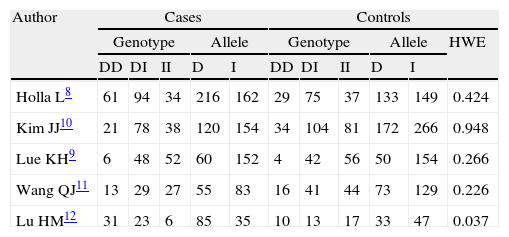
ResultsStudy characteristicsThere were 10 papers relevant to the literature search strategy. Based on the inclusion criteria, we only identified five case-control studies (four from East Asia and one from Europe) which evaluated the association between ACE gene I/D polymorphism and AR risk.8–12 The characteristics of the included studies are summarised in Table 1. All included studies extracted DNA from peripheral blood and used Rigat polymerase chain reaction (PCR) and triple-primer PCR for genotyping.13 However, only one study mentioned quality control on genotyping by the method of Shanmugam et al.14 These studies included 561 AR cases and 603 healthy controls. The genotype distribution among the control of the study by Lu HM et al. was not consistent with HWE.12 Finally, we further pooled and analysed the remaining four studies. The distribution of ACE genotypes and allelic frequencies in the studies are summarised in Table 2.
Characteristics of all included studies.
| Author | Year | Country | Ethnicity | Subjects, n (M/F) | Genotyping methods | |
| Cases | Controls | |||||
| Holla L8 | 1999 | Czech | Caucasian | 189 (–/–) | 141 (74/67) | Rigat-PCR (quality control on genotyping) |
| Kim JJ10 | 2004 | Korea | East Asian | 137 (72/65) | 219 (121/98) | Triple-primer PCR |
| Lue KH9 | 2006 | Taiwan | East Asian | 106 (68/38) | 102 (50/52) | Rigat-PCR |
| Wang QJ11 | 2005 | China | East Asian | 69 (27/42) | 101 (55/46) | Rigat-PCR |
| Lu HM12 | 2006 | China | East Asian | 60 (23/37) | 40 (22/18) | Rigat-PCR |
Distribution of ACE allele and genotype in all included studies.
| Author | Cases | Controls | |||||||||
| Genotype | Allele | Genotype | Allele | HWE | |||||||
| DD | DI | II | D | I | DD | DI | II | D | I | ||
| Holla L8 | 61 | 94 | 34 | 216 | 162 | 29 | 75 | 37 | 133 | 149 | 0.424 |
| Kim JJ10 | 21 | 78 | 38 | 120 | 154 | 34 | 104 | 81 | 172 | 266 | 0.948 |
| Lue KH9 | 6 | 48 | 52 | 60 | 152 | 4 | 42 | 56 | 50 | 154 | 0.266 |
| Wang QJ11 | 13 | 29 | 27 | 55 | 83 | 16 | 41 | 44 | 73 | 129 | 0.226 |
| Lu HM12 | 31 | 23 | 6 | 85 | 35 | 10 | 13 | 17 | 33 | 47 | 0.037 |
D, deletion, I, insertion.
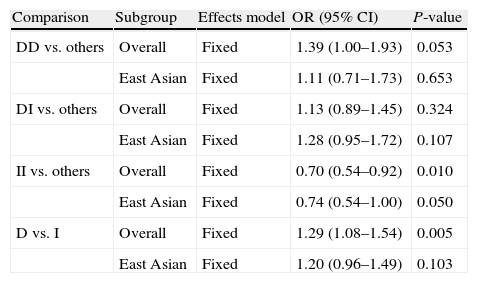
The combined results of ACE gene I/D polymorphism and AR risk can be seen in Table 3. The results indicated an association between ACE gene I/D polymorphism and AR risk in the overall analysis using the fixed-effects model (II vs. others: OR=0.70, 95% CI=0.54–0.92, P=0.010; D vs. I: OR=1.29, 95% CI=1.08–1.54, P=0.005).
Meta-analysis of ACE polymorphisms and the risk of AR.
| Comparison | Subgroup | Effects model | OR (95% CI) | P-value |
| DD vs. others | Overall | Fixed | 1.39 (1.00–1.93) | 0.053 |
| East Asian | Fixed | 1.11 (0.71–1.73) | 0.653 | |
| DI vs. others | Overall | Fixed | 1.13 (0.89–1.45) | 0.324 |
| East Asian | Fixed | 1.28 (0.95–1.72) | 0.107 | |
| II vs. others | Overall | Fixed | 0.70 (0.54–0.92) | 0.010 |
| East Asian | Fixed | 0.74 (0.54–1.00) | 0.050 | |
| D vs. I | Overall | Fixed | 1.29 (1.08–1.54) | 0.005 |
| East Asian | Fixed | 1.20 (0.96–1.49) | 0.103 |
D, deletion, I, insertion.
Since there was only one study involving Caucasians, we finally carried out the further analysis of the East Asians. The results showed no significant association between all genotypes and AR risk in East Asians (DD vs. others: OR=1.11, 95% CI=0.71–1.73, P=0.653; DI vs. others: OR=1.28, 95% CI=0.95–1.72, P=0.107; II vs. others: OR=0.74, 95% CI=0.54–1.10, P=0.050) (Table 3 and Fig. 1). In addition, the allele D was not associated with AR risk in East Asians (OR=1.20, 95% CI=0.96–1.49, P=0.103) (Table 3 and Fig. 1).
Sensitivity analysis and publication bias DD vs. others; (b) ID vs. others; (c) II vs. others; (d) D vs. I polymorphisms in East Asians. The squares and horizontal lines correspond to the OR and 95% CI. OR, odds ratio; 95% CI, 95% confidence interval.")
We carried out the sensitivity analysis by sequentially omitting a single study. The magnitude of effect in overall analysis and subgroup analysis was not excessively influenced. Publication bias of the included studies was assessed by the funnel plot and the Egger test. The funnel plot was symmetrical and there was no apparent evidence of publication bias (Fig. 2).
Discussion. The horizontal and vertical axes correspond to the logOR and SE(logOR). OR, odds ratio; SE, standard error.")
AR may be a multifactorial disease. Some studies have shown that a combination of genetic susceptibility and environmental factors can ultimately induce the occurrence of this disease.15,16 Several susceptibility genes including ACE gene were considered to be associated with the risk of AR.17 ACE gene I/D polymorphism can strongly affect the plasma and cellular ACE activity level.18–20 Average ACE activity level in people with the DD carriers is approximately twice that in the II genotype subjects. The individuals with ID genotype have intermediate levels. It is likely that the down-regulation in ACE levels with the II genotype might increase bradykinin and trigger the inflammatory response. It is frequently reported that ACE inhibitors could induce cough in patients with heart failure or hypertension. These potential mechanisms may be involved in the sensitisation of sensory nerves and the enhancement of the cough reflex in airway by the bradykinin.21 Therefore, ACE gene I/D polymorphism may play a vital role in airway remodelling in AR.
Previous studies have investigated the association between ACE gene I/D polymorphisms and the risk of AR. Lue KH et al.9 found that ACE DD genotype might play a role in the development of the asthma phenotype in Taiwanese children with allergic rhinitis. However, other studies indicated that polymorphisms in the ACE gene may not be related to the development of allergic rhinitis in the Korean and the mainland Chinese populations.10,11 In Caucasian, Holla L's study inference on ACE DD genotype was consistent with the results of Lue KH, meanwhile they also reported that the D allele may also be a risk factor for development of AR.8
In the current study, we pooled and analysed these data including 561 cases and 603 controls from East Asia and Europe. The results showed that the ACE gene I/D polymorphisms were not associated with the risk of AR in East Asians.
We noted another large sample meta-analysis about the associations between the ACE gene I/D polymorphisms and asthma risk.6 The results of this study showed the DD homozygote carrier was associated with the risk of asthma in Asians but not in Caucasians. Their results were obviously not consistent with our study. Therefore, although asthma and AR have been considered to be atopic disease, two kinds of disease may have different aetiologies and genetic basis. In addition, the number of included studies also restricts the results of our study. In particular the study on the Caucasian race was limited and we could not include black African populations.
There are other potential limitations in our study. In this study we assessed the publication bias using funnel plots. Although we could not find significant publication bias, it only showed a possible trend, the results of our study should be interpreted with caution because the number of included studies is limited.22 Therefore large sample studies will be necessary to explore the association between ACE gene I/D polymorphisms and the risk of AR. On the other hand, our study only focused on the relationships between ACE gene I/D polymorphisms and AR susceptibility; we could not evaluate the association between ACE gene I/D polymorphisms and the severity of AR, because the included studies did not mention those relevant data.
ConclusionThe present study shows that ACE gene I/D polymorphisms were not associated with the risk of AR in East Asians. These results need to be confirmed in future studies.
Ethical disclosuresProtection of human subjects and animals in researchThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Conflict of interestSupported by the Natural Science Fund of Yunnan Province (No. 2013FB044) and the Joint Foundation of Science and Technology Department of Yunnan Province and Kunming Medical University (No. 2010CD223). We state explicitly there no potential conflicts exist.
