






The AEU Guidelines of 2017 consider laparoscopic and robot-assisted approaches as investigational procedures. The surgical learning curve is defined as the minimum number of cases that a surgeon has to perform in order to reproduce a technique considered as standard.
The aim of this study is to analyze, within our department, the implementation of a laparoscopic radical cystectomy (LRC) program compared with a well consolidated and standardized open radical cystectomy (ORC) program.
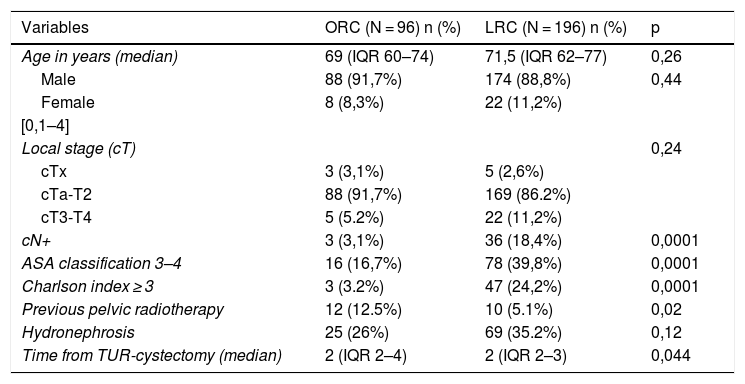
Material and methodsRetrospective cohort analysis of two cystectomy groups: LRC (n = 196) (20062016) vs ORC (n = 96) (2003–2005).
Comparison of the evolution over time of the following parameters: operative time, blood transfusion rates, resection margins, postoperative complications, hospital stay and recurrence.
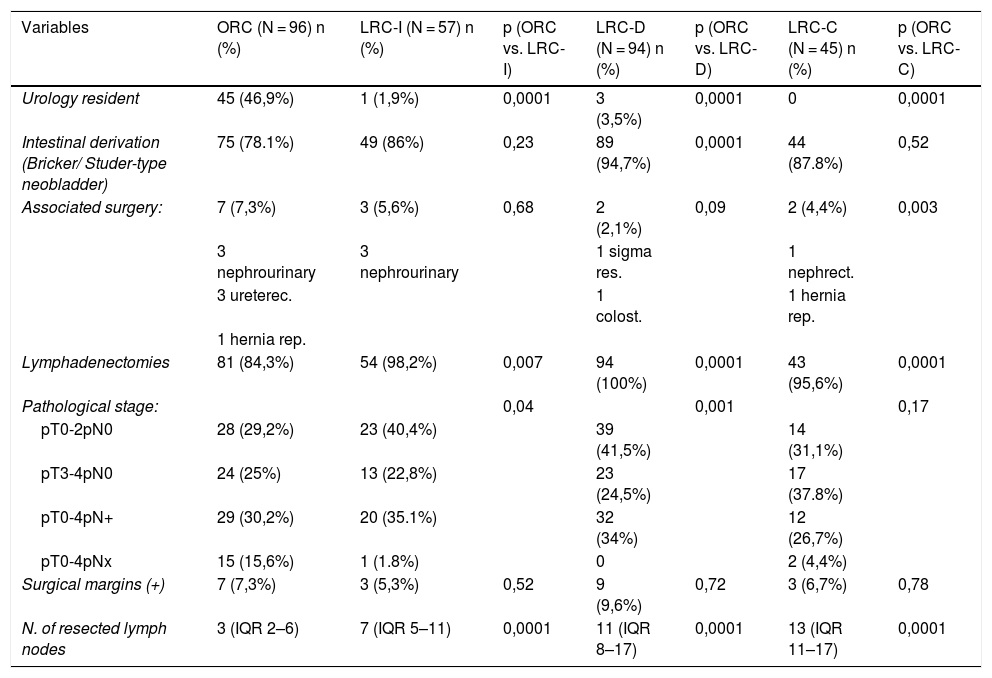
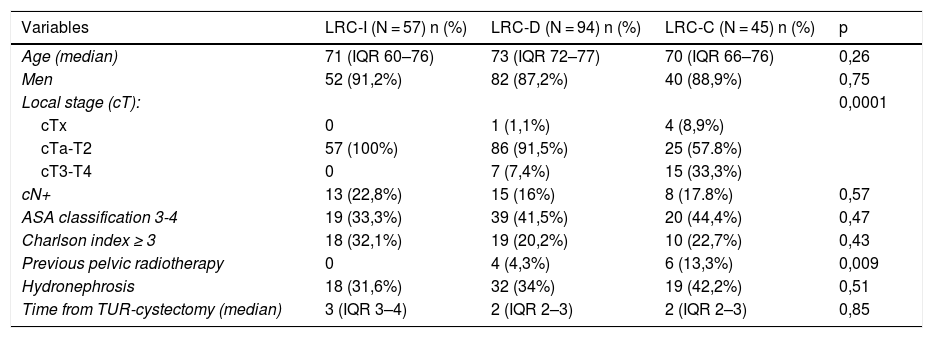
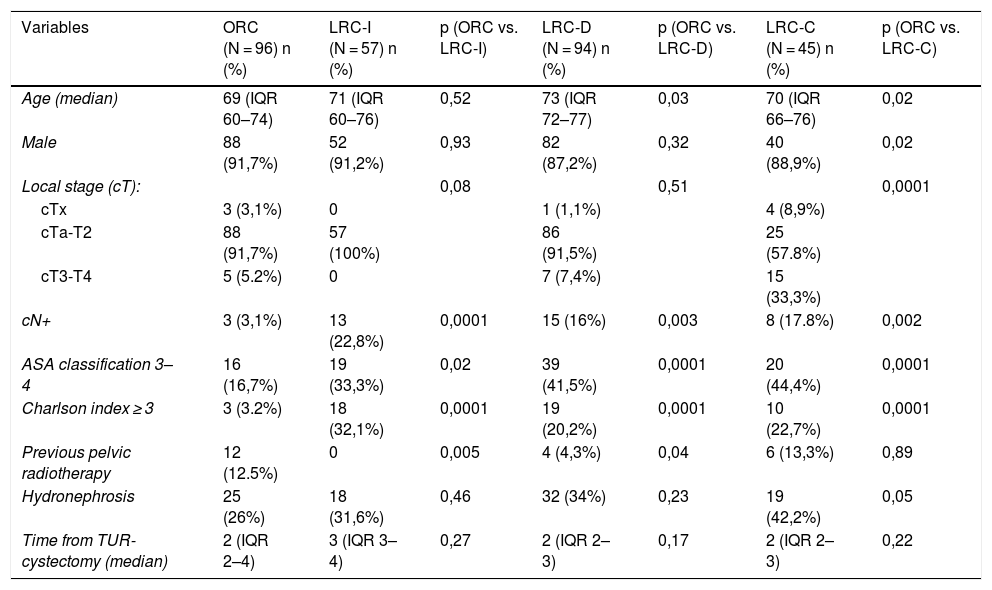
Three time periods have been defined for LRC: implementation (2006–09) (LRC-I), development (2010–14) (LRC-D) and consolidation (2015–16) (LRC-C); comparing each of them with the control group (ORC).
The chi-square test was used for the comparison of the qualitative variables and the Anova test for the numerical ones.
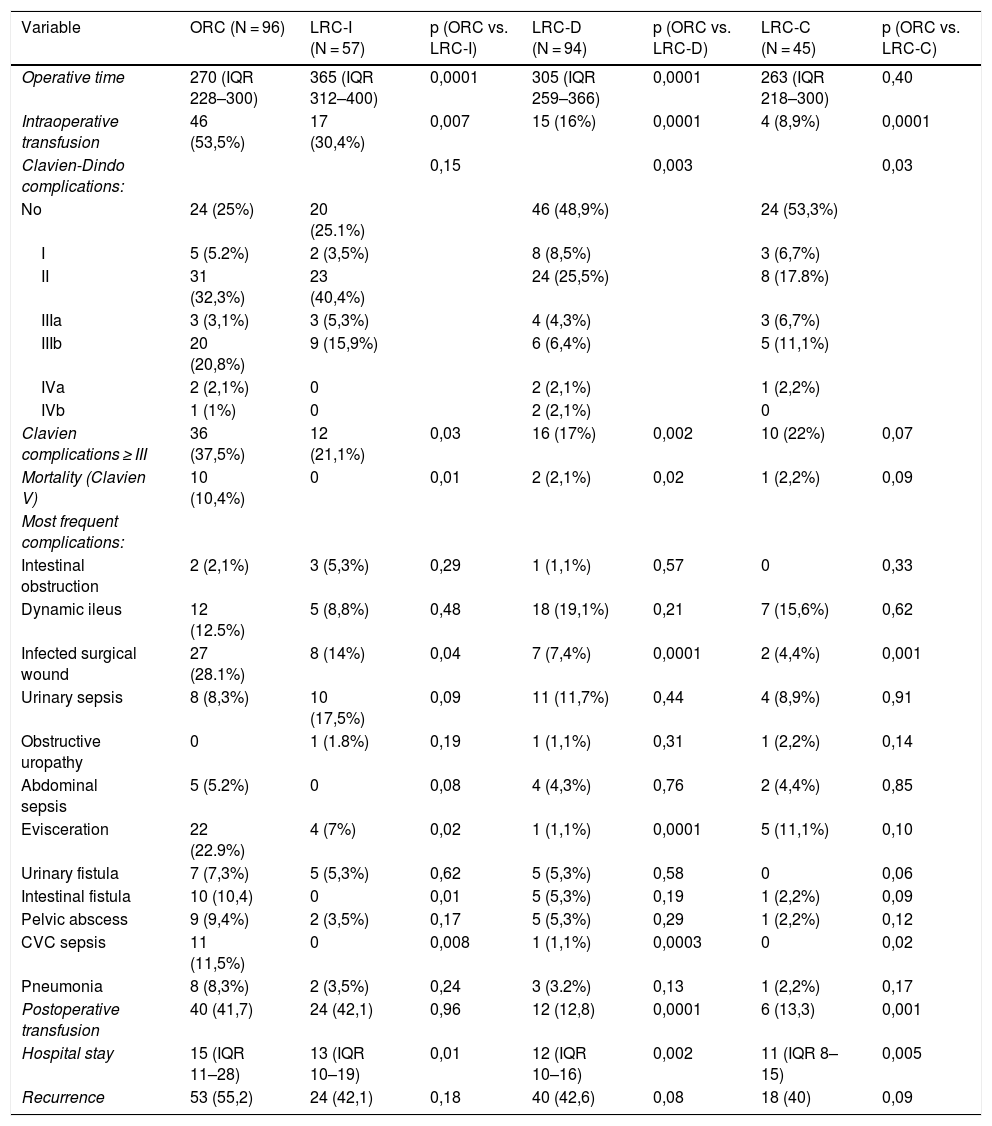
ResultsWhen compared to ORC, LRC presented longer operative times in LRC-I and LRC-D periods. We observed a trend toward shorter operative time than ORC in the consolidation period (LRC-C).
LRC also presented lower intraoperative transfusion rates in all periods and lower postoperative rates in CRL-D and CRL-C. Overall complications in LRC-D and LRC-C were lower in LRC, having fewer major complications (Clavien ≥ 3) in the 3 periods. A decrease in mortality and hospital stay after the LRC-I phase was also observed. These results were consolidated during the two last periods of the study.
We have not observed significant differences between ORC and LRC when comparing surgical margins and recurrence rates, neither in the total series, nor in the comparison between the different periods. These results endorse the oncologic safety of LRC from the beginning of the implementation process.
ConclusionsWhen compared to ORC, LRC improves perioperative transfusion rates, complications and hospital stay from its implementation period, maintaining oncological safety. On the contrary, longer operative times during implementation and development were observed. However, in our series, we observed a trend toward shorter operative times than ORC approach in the consolidation period. We have validated the laparoscopic approach for radical cystectomy in our service.
Las Guidelines de la AEU de 2017, consideran el acceso laparoscópico o asistido por robot como procedimientos en investigación. La curva de aprendizaje se define por el número mínimo de casos que es necesario realizar para reproducir la técnica considerada como estándar.
El objetivo de este estudio es analizar en el mismo servicio, la implantación de un programa de cistectomía laparoscópica (CRL), comparándolo con un programa consolidado y estandarizado de cistectomía abierta (CRA).
Material y métodoAnálisis de cohortes retrospectivo de dos grupos de cistectomías: CRL (n = 196) (2006–2016) frente a CRA (n = 96) (2003–2005).
Comparación de la evolución en el tiempo de los siguientes parámetros: tiempo quirúrgico, las necesidad de transfusión, el estado de los márgenes quirúrgicos de resección, las complicaciones postoperatorias, la duración de la estancia hospitalaria y las recidivas.
Se han definido 3 periodos de tiempo para CRL: implantación (2006–09) (CRLI), desarrollo (2010–14) (CRL-D) y consolidación (2015–16) (CRL-C); comparándose cada uno de ellos con el grupo control (CRA).
Para el contraste de variables cualitativas se ha utilizado el test de la Chi cuadrado y para las variables numéricas el test de Anova.
ResultadosLa CRL, en comparación con la CRA, presentó un mayor tiempo quirúrgico en las fases de CRL-I y CRL-D, observando una tendencia de menores tiempos operatorios que la CRA en el periodo de consolidación.
La CRL presenta además menor trasfusión intraoperatoria en los 3 periodos y postoperatoria en CRL-D y CRL-C, menos complicaciones totales en CRL-D y CRL-C, menos complicaciones graves(Clavien ≥ 3) en las 3 fases; así como una disminución de la mortalidad y estancia hospitalaria desde la fase de CRL-I, consolidándose esta disminución en los otros dos periodos de estudio.
No hemos observado diferencias significativas entre CRA y CRL en cuanto a márgenes quirúrgicos y recurrencias ni en el total de la serie ni en la comparación entre los distintos periodos, lo que avala la seguridad de la CRL, desde su inicio.
ConclusionesLa CRL frente a CRA mejora desde su implantación el porcentaje de transfusiones, de complicaciones y la estancia hospitalaria, con seguridad oncológica, a expensas de un mayor tiempo quirúrgico en las fases de implantación y desarrollo. Sin embargo, en nuestra serie observamos una tendencia de menores tiempos quirúrgicos que la CRA en el periodo de consolidación. En nuestro servicio el abordaje laparoscópico se ha validado en el tratamiento de la cistectomía radical.
