






Recurrence trends after renal cell cancer (RCC) nephrectomy are not clearly defined.
ObjectiveTo evaluate recurrence trends according to recurrence risk groups (RRG).
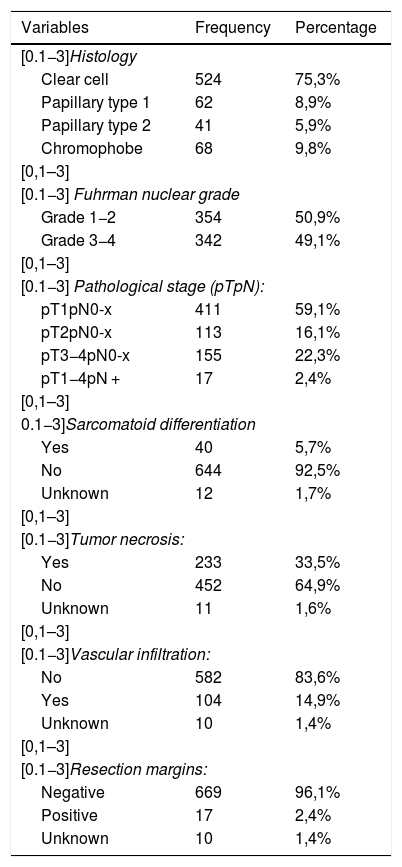
MethodsRetrospective analysis of 696 patients with RCC treated with nephrectomy between 1990−2010.
Three RRG were defined according to the presence of anatomopathological variables (pTpN stage, nuclear grade, tumor necrosis (TN), sarcomatoid differentiation (SD), positive resection margin (RM)):
- Low RG (LRG):pT1pNx-0 G1–4, pT2pNx-0 G1–2; no TN, SD and/or RM(+)
- Intermediate RG (IRG):pT2pNx-0 G3–4;pT3–4pNx-0 G1–2; LRG with TN.
- High RG (HRG):pT3–4pNx-0 G3–4;pT1–4pN+;IRG with TN and/or SD; LRG with SD and/or RM (+).
The Kaplan-Meier method has been used to evaluate recurrence-free survival as a function of RRG. The log-rank test was used to evaluate differences between survival curves.
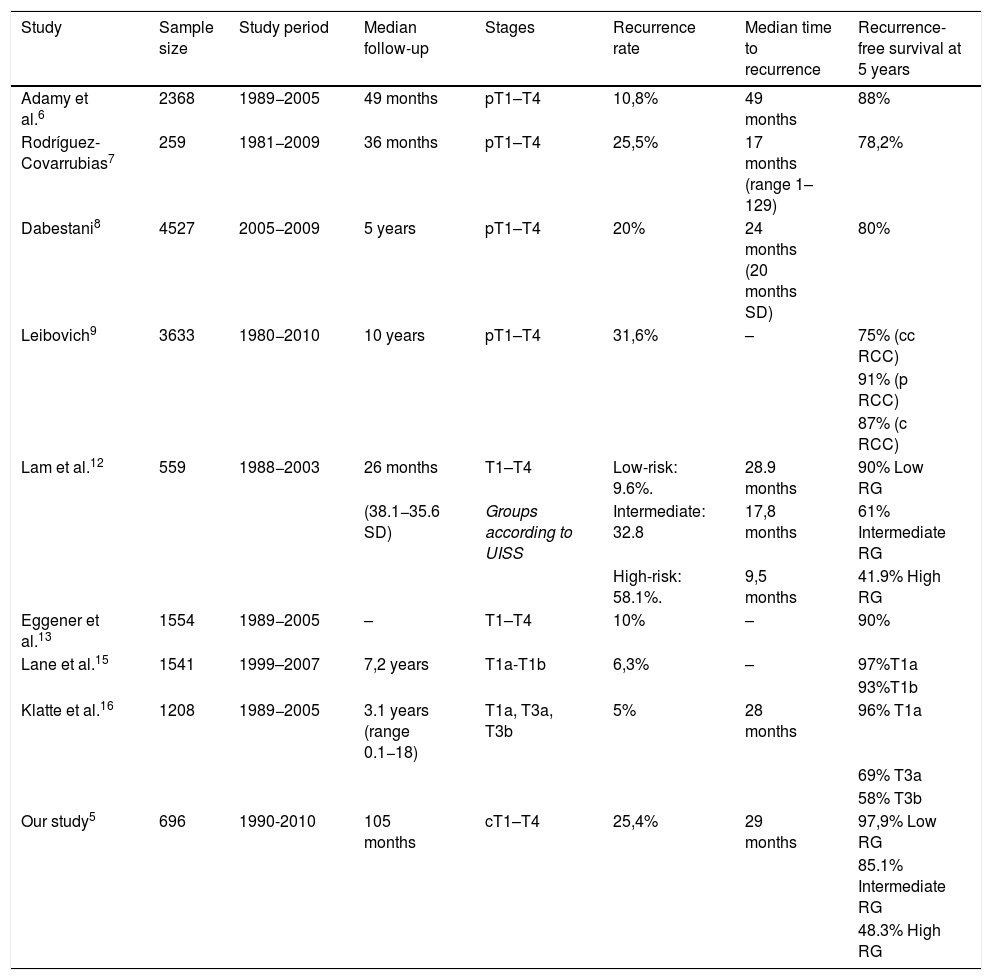
ResultsThe median follow-up was 105 (IQR 63–148) months. Of the total series, 177 (25.4%) patients presented recurrence: distant 15.9%, local 4.9% and 4.6% distant and local.
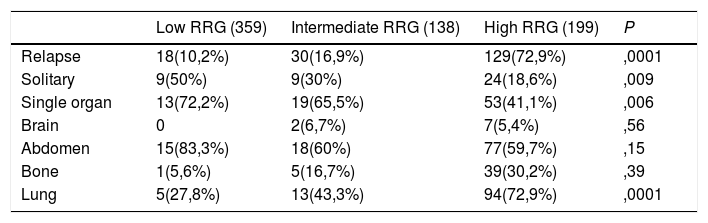
The recurrence rate varied according to the RRG with values of 72.9% for HRG, 16.9% for IRG and 10.2% for LRG (P = .0001). Most cases in LRG presented single organ recurrence (72.2%) (P = .006). The LRG experienced recurrence as single metastasis in 50% of cases, compared to 30% and 18.6% in IRG and HRG, respectively (P = .009).
The most common sites of recurrence were lung and abdomen. Lung recurrence predominated in the HRG (72.9%) (P = .0001) and abdominal, in the LRG (83.3%) with a tendency to significance (P = .15).
ConclusionsRecurrence rates (especially bone and lung) increase with higher RG. Single organ recurrences and single metastases are more frequent in LRG.
No están claramente definidos los patrones de recurrencia tras nefrectomía por cáncer renal(CCR).
ObjetivoEvaluar patrones de recidiva en función del grupo de riesgo de recurrencia(GRR).
Material y métodoAnálisis retrospectivo de 696 pacientes con CCR tratados con nefrectomía entre 1990−2010.
Se definieron tres GRR según la presencia de variables anatomopatológicas (estadio pTpN, grado nuclear, necrosis tumoral (NT), diferenciación sarcomatoide (DS), margen de resección positivo (MR)):
- GR bajo (GRB): pT1pNx-0 G1–4, pT2pNx-0 G1–2; no NT,DS y/o MR(+)
- GR Intermedio(GRI):pT2pNx-0 G3–4;pT3–4pNx-0 G1–2; GRB con NT.
- GR alto (GRA): pT3–4pNx-0 G3–4;pT1–4pN+;GRI con NT y/o DS; GRB con DS y/o MR (+).
Para el contraste de variables cualitativas se utilizó el test de la Chi cuadrado.El método de Kaplan-Meier se ha utilizado para evaluar la supervivencia libre de recidiva en función de los GRR. Para evaluar diferencias entre las curvas de supervivencia se ha utilizado el test de log-rank.
ResultadosLa mediana de seguimiento fue de 105(IQR 63–148) meses. Del total de la serie recidivaron 177(25,4%) pacientes: 15,9% a distancia, 4,9% local y 4,6% a distancia y local.
La tasa de recurrencia varió según el GRR con tasas del 72,9% en GRA, 16,9% en GRI y 10,2% en GRB(P = ,0001). La recurrencia en órgano único fue mayoritaria en el GRB (72,2%)(P = ,006). El GRB presentó recidiva en forma de metástasis única en el 50% de los casos, frente al 30% y 18,6% en GRI y GRA, respectivamente (P = ,009).
Las localizaciones de recurrencia más habituales fueron pulmón y abdomen. La localización pulmonar predominó en el GRA(72,9%)( P = ,0001) y la abdominal en el GRB(83,3%) con una tendencia a la significación(P = ,15).
ConclusionesA medida que aumenta el grupo de riesgo aumentan las recurrencias, sobre todo óseas y pulmonares. En el GRB son más frecuentes las metástasis únicas y en órgano único.
