




To present the 2011 European Association of Urology (EAU) guidelines on non-muscle-invasive bladder cancer (NMIBC).
Evidence acquisitionLiterature published between 2004 and 2010 on the diagnosis and treatment of NMIBC was systematically reviewed. Previous guidelines were updated, and the level of evidence and grade of recommendation were assigned.
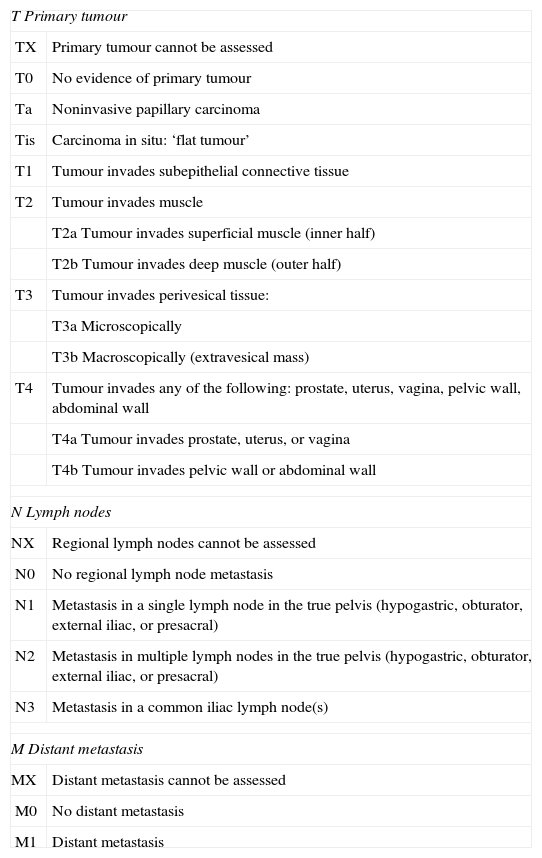
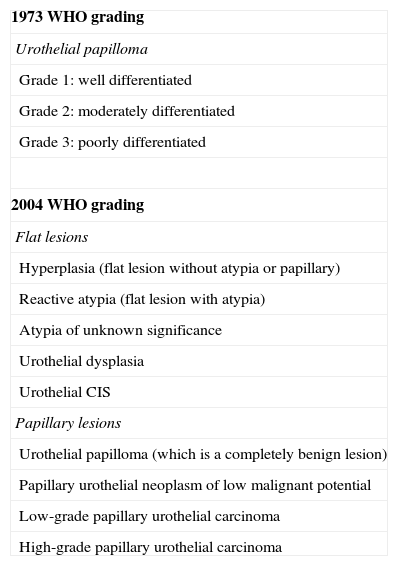
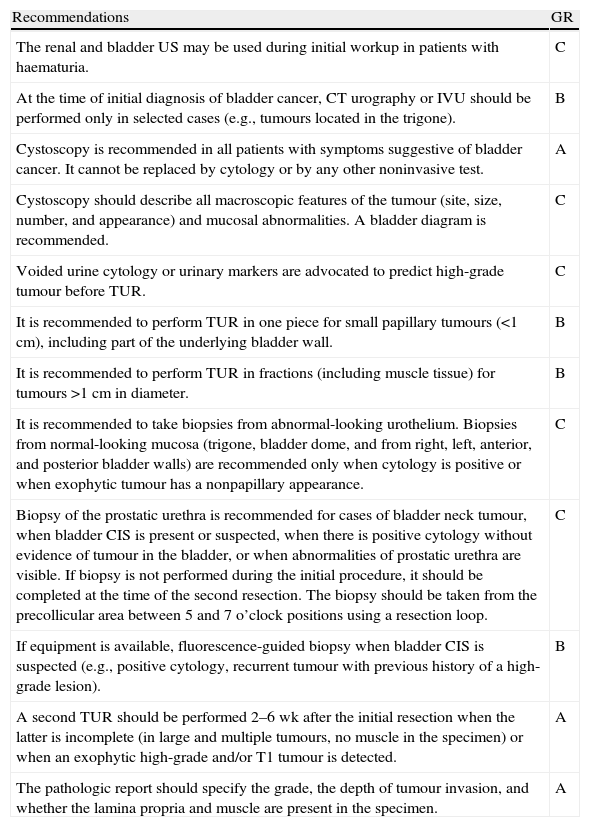
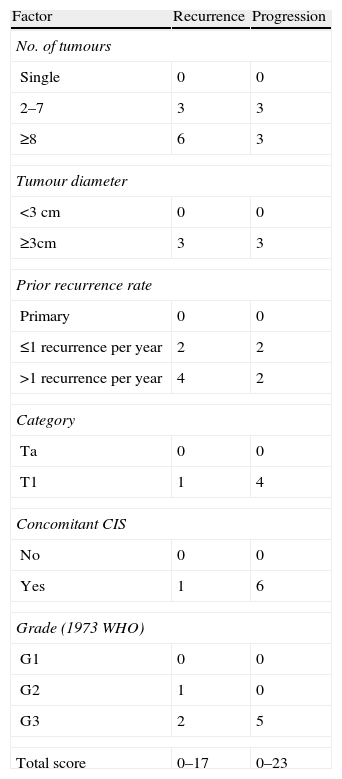
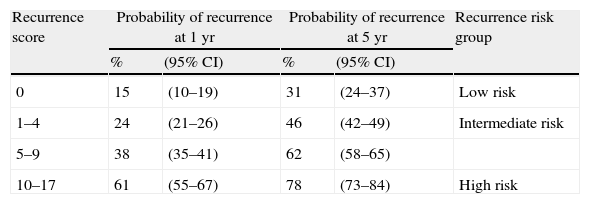
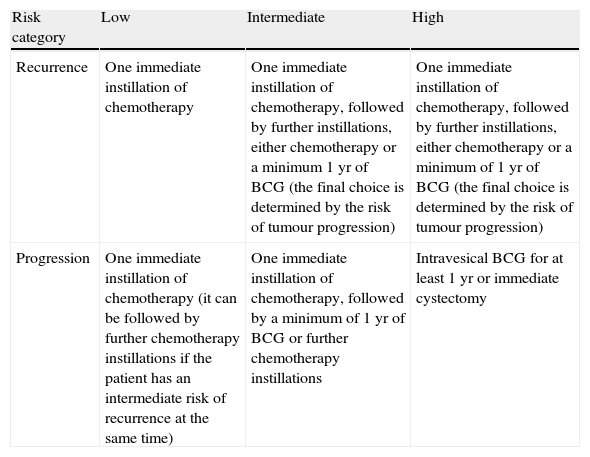
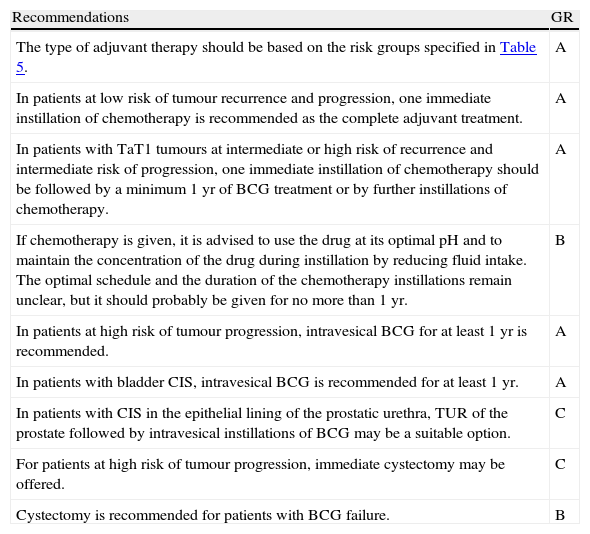
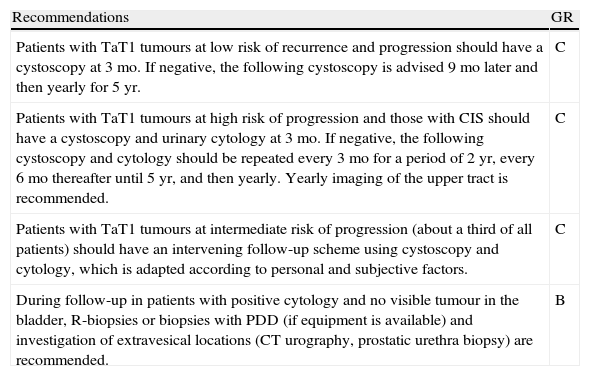
Evidence synthesisTumours staged as Ta, T1, or carcinoma in situ (CIS) are grouped as NMIBC. Diagnosis depends on cystoscopy and histologic evaluation of the tissue obtained by transurethral resection (TUR) in papillary tumours or by multiple bladder biopsies in CIS. In papillary lesions, a complete TUR is essential for the patient's prognosis. Where the initial resection is incomplete or where a high-grade or T1 tumour is detected, a second TUR should be performed within 2–6 wk. In papillary tumours, the risks of both recurrence and progression may be estimated for individual patients using the scoring system and risk tables. The stratification of patients into low-, intermediate-, and high-risk groups (separately for recurrence and progression) is pivotal to recommending adjuvant treatment. For patients with a low risk of tumour recurrence and progression, one immediate instillation of chemotherapy is recommended. Patients with an intermediate or high risk of recurrence and an intermediate risk of progression should receive one immediate instillation of chemotherapy followed by a minimum of 1 yr of bacillus Calmette-Guérin (BCG) intravesical immunotherapy or further instillations of chemotherapy. Papillary tumours with a high risk of progression and CIS should receive intravesical BCG for 1 yr. Cystectomy may be offered to the highest risk patients, and it is at least recommended in BCG failure patients.
ConclusionsThese abridged EAU guidelines present updated information on the diagnosis and treatment of NMIBC for incorporation into clinical practice.
Presentar la guía clínica de la Asociación Europea de Urología (EAU) de 2011 del carcinoma de vejiga no músculo-invasivo (CVNMI).
Adquisición de la evidenciaSe ha realizado una revisión sistemática de la literatura publicada entre 2004 y 2010 acerca del diagnóstico y el tratamiento del CVNMI. Se actualizaron las guías clínicas previas, y se asignó un nivel de evidencia (NE) y un grado de recomendación (GR).
Síntesis de la evidenciaLos tumores en estadio Ta, T1 o carcinoma in situ (CIS) se agrupan como CVNMI. El diagnóstico depende de la cistoscopia y de la evaluación histológica del tejido obtenido por resección transuretral (RTU) en los tumores papilares o por biopsias de vejiga múltiples en el CIS. En las lesiones papilares, una completa RTU es esencial para el pronóstico del paciente. Cuando la primera resección es incompleta o cuando se detecta un tumor de alto grado o T1, se debe realizar una segunda RTU a las 2-6 semanas. En los tumores papilares, el riesgo tanto de recurrencia como de progresión se puede calcular de manera individual mediante los sistemas de puntuación y tablas de riesgo. La estratificación de los pacientes en grupos de riesgo bajo, intermedio y alto (separando la recidiva y la progresión) es fundamental para recomendar un tratamiento adyuvante. Para los pacientes con bajo riesgo de recurrencia y progresión se recomienda una instilación inmediata de quimioterapia. Los pacientes con riesgo intermedio o alto de recurrencia y riesgo intermedio de progresión deben recibir una instilación inmediata de quimioterapia seguida de un mínimo de un añno con inmunoterapia intravesical con bacilo de Calmette-Guérin (BCG) o más instilaciones de quimioterapia. Los tumores papilares con alto riesgo de progresión y CIS deben recibir BCG intravesical durante un año. Se puede ofrecer una cistectomía a los pacientes de más alto riesgo, y por lo menos se recomienda a los pacientes en los que ha fallado la BCG.
ConclusionesLa versión reducida de esta guía clínica de la EAU presenta una información actualizada sobre el diagnóstico y el tratamiento del CVNMI para la incorporación a la práctica clínica.
