


Tipping, mesiodistal root inclination, torque and in-out movements; they are information prescribed in the bracket. They locate the tooth in the three planes of space; it is thought that by filling the slot, expression of the prescription is obtained. Prescription provides specific measurements of tipping to distribute forces adequately on the long axis of the tooth thus resulting in treatment stability and health of the stomatognathic system. When these conditions are not obtained, trauma might develop (widening of the periodontal space, root resorption, bone defects).
ObjectiveTo compare tipping expression before and during treatment as well as the trans-treatment tipping against the one established by MBT and Roth prescriptions.
MethodsPre and trans-treatment tipping was evaluated in panoramic radiographs (n = 60) from the angle formed by a baseline (infraorbital axis) and the long axis of the tooth in the upper arch, premolar to premolar. The comparison of the pre and trans-treatment tipping was performed per tooth and per group (central, lateral, canines, premolars). Student's T test and a one-sample T test were used to compare the values obtained by group against the values of each prescription.
ResultsTrans-treatment tipping was affected in a negative way in most of the teeth; except in the canines, which are affected in a positive way (p < 0.05, in OD 15, 23, 24 and 25). The posterior left segment was the most affected in a negative way, with differences between 4-6°. The incisors maintained their pre-treatment tipping. With regard to the comparison of trans-treatment tipping for each prescription, it was observed that in no case the set value was obtained, with differences of 4-6° for central incisors and premolars and 8-11° for canines and lateral incisors (p < 0.05 in all groups with both techniques).
ConclusionTrans-treatment tipping is affected in a negative way in the posterior segment. The anterior sector is more stable, while the canines are favored with regard to the increase of distal tipping. In spite of the premise that pre-adjusted appliances optimize orthodontic treatment, human error or the clinician's ability remains a relevant factor for success.
Tipping, inclinación mesiodistal radicular, torque y movimientos in-out; son información prescrita en el bracket, ubican al diente en los tres planos del espacio, se piensa que llenando el slot, se obtiene la expresión de la prescripción. Éstas establecen medidas específicas de tipping para brindar una adecuada distribución de fuerzas sobre el eje longitudinal dental resultando en estabilidad del tratamiento y salud del complejo estomatognático. De no ser obtenido esto, podría desarrollarse un trauma oclusal (ensanchamiento del espacio periodontal, reabsorción radicular, defectos óseos).
ObjetivoComparar la expresión del tipping pre- y transtratamiento así como el tipping-transtratamiento contra el establecido por las prescripciones MBT y Roth.
MetodologíaEl tipping pre- y transtratamiento fue evaluado en radiografías panorámicas (n = 60) a partir del ángulo formado por línea base (eje infraorbitario) y el eje longitudinal dental en la arcada superior, premolar-premolar. La comparación del tipping pre- y transtratamiento se realizó por diente y grupo (centrales, laterales, caninos, premolares). Se utilizó la prueba de t Student pareada y prueba t de una muestra para comparar los valores obtenidos por grupo contra los valores de cada prescripción.
ResultadosEl tipping transtratamiento se vio afectado de manera negativa en la mayoría de los dientes; excepto en caninos los cuales se afectaron de manera positiva, (p < 0.05, en OD 15, 23, 24 y 25). El sector posterior izquierdo fue el más afectado de manera negativa, con diferencias entre 4-6°. Los incisivos mantienen su tipping pretratamiento. En cuanto a la comparación tipping transtratamiento contra cada prescripción, se observa que en ningún caso se obtiene el valor establecido, con diferencias de 4-6° para centrales y premolares; y de 8-11° para caninos y laterales (p < 0.05 en todos los grupos con ambas técnicas).
ConclusiónEl tipping transtratamiento se ve afectado de manera negativa en sectores posteriores, el sector anterior se muestra más estable, mientras que los caninos se ven favorecidos con respecto al aumento de tipping distal. A pesar de la premisa de que la aparatología preajustada optimiza el tratamiento de ortodoncia, el error humano o habilidad del clínico siguen siendo factores relevantes para el éxito, presentando detalles por mejorar y cuestiones biológicas a considerar
Pre-adjusted appliances have provided benefits to orthodontics in order to achieve a better finishing under the premise of a reduced treatment time and a smaller number of bends in the archwire unlike the standard or edgewise appliances.1 It is thought that if the bracket is placed in the correct or ideal position then it would express the prescribed information (tip, torque and in-out movements) just by increasing the archwire size until the slot is filled entirely.
Over time there have been some changes to both the requirements of the appliances as well as in the ideal position for the bracket with the purpose of optimizing orthodontic treatment. For example in 1928, Angle recommended as an ideal position for the bracket the center of the labial surface of the tooth crown;2 Begg in 1973 established preset heights on the basis of the incisal edge; by 1976, Andrews suggested placing the bracket at the intersection of the mid-point of the length of the clinical crown and the mid-point of Andrews facial axis;3 whereas in 1995 McLaughlin and Bennet recommended to place the bracket at a measured distance from the incisal edge with different vertical positions depending on the size of the teeth.1
There has been much debate on what school of thought is the ideal or which presents better results. Investigations such as those made by Fukuyo K. and Armstrong D,4–8 have shown that there are no statistically significant differences between bonding at the center of the clinical crown, respecting the different levels of the marginal crests of premolars or the parameter of the distances from the incisal edge.
There are many issues that interfere in obtaining optimum results from orthodontic treatment. Some of them are: variations in dental anatomy,7 facial biotype, shape and disposition of the mesh the bracket and the difference in manufacturing tolerances between slot size and archwires.6 Due to these complications several alternatives have arisen to eliminate bonding error and allow the total expression of the prescription with regard to tipping, torque and in-outmovements. Studies such as the one performed by Joiner,9 in which indirect bonding was assessed, concluded that due to a better visual access and working time in the laboratory, indirect bonding presents better results for fixed appliances placement, although not precisely reflected in the decrease of bends in the archwire.
Anatomic variations regarding crown convexities and heights are factors that have also been analyzed, however as denoted already in a study by Park D et al.10 no improvements have been achieved completely in those aspects that interfere with the full expression of the prescription.
However, it has been observed that regardless of the prescription, bonding errors continue to be present such as human error or lack of skill from the operator.6,11 It is believed that all the abovementioned factors are present because the reference point is always the clinical crown without considering the tooth jointly with the location or distribution of its root and surrounding structures.12
With the intention of evaluating the premise that pre-adjusted appliances provide benefits to orthodontics such as better finishing in less time and with fewer compensation bends in the archwire, the objective of this study was to compare radiographically mesiodistal root inclination or tipping before treatment (pre-treatment) and the one obtained from orthodontic treatment prior to finishing with compensation bends or before detailing (trans-treatment), as well as to compare the tipping obtained at trans-treatment with the values set by the prescriptions (MBT and Roth).
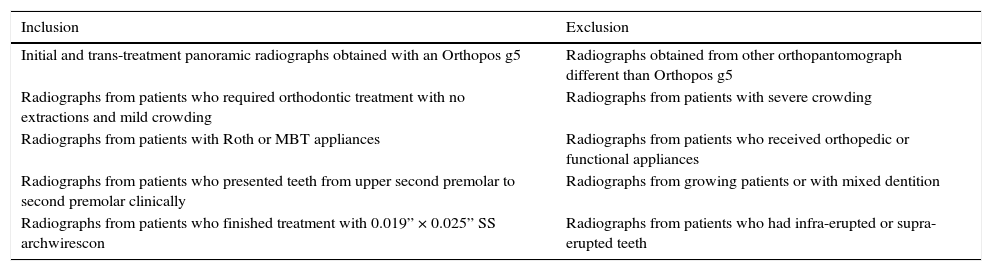
MATERIAL AND METHODSClinical records of patients who requested dental care at the Department of Orthodontics of the Division for Pos-graduate Studies and Research of the UNAM, during the period 2010-2012 were analyzed. A sample of 120 panoramic radiographs obtained with g5 Orthopos (Dental Sirona System Australia) was selected from 60 patients who received orthodontic treatment without extractions; 60 were the initial radiographs and 60 correspond to the time before bracket repositioning or compensation bends. Inclusion and exclusion criteria are shown in table I.
Inclusion and exclusion criteria.
| Inclusion | Exclusion |
|---|---|
| Initial and trans-treatment panoramic radiographs obtained with an Orthopos g5 | Radiographs obtained from other orthopantomograph different than Orthopos g5 |
| Radiographs from patients who required orthodontic treatment with no extractions and mild crowding | Radiographs from patients with severe crowding |
| Radiographs from patients with Roth or MBT appliances | Radiographs from patients who received orthopedic or functional appliances |
| Radiographs from patients who presented teeth from upper second premolar to second premolar clinically | Radiographs from growing patients or with mixed dentition |
| Radiographs from patients who finished treatment with 0.019” × 0.025” SS archwirescon | Radiographs from patients who had infra-erupted or supra-erupted teeth |
Once the sample was obtained, the pre and trans treatment radiographs of the 60 patients were assigned a random number for the pre and trans tipping expression comparison.
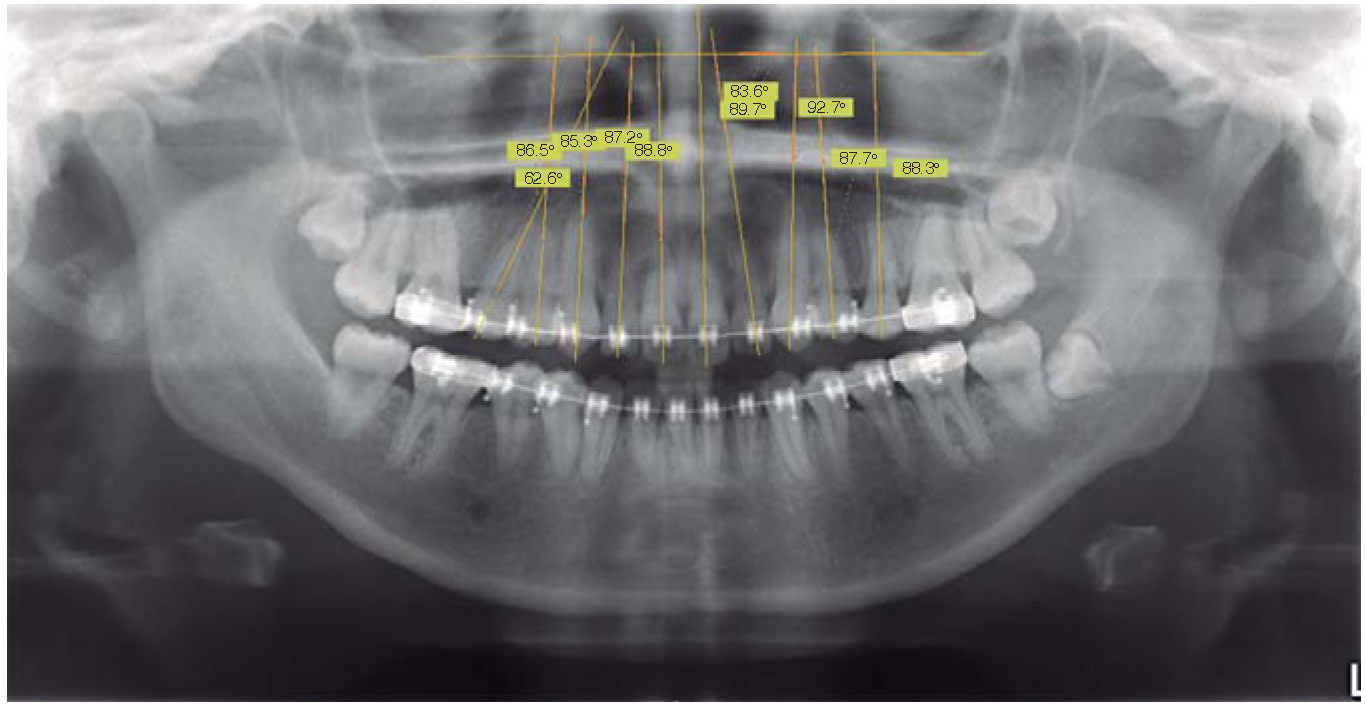
Tracing methodThe infraorbital axis was determined as a fixed structure for the upper arch. Subsequently, the long axis of the teeth was traced from upper second premolar to second premolar.
With the help of the SIDEXIS XG/Sirona Dentalprogram, the measurements were obtained. Three measurements were performed for each tooth to obtain the mean.
The distal angles formed by the longitudinal axis of each tooth were measured against the infraorbital axis as shown in figure 1.
Statistical analysis
The Kolmogorov-Smirnov test was conducted to test the data's normality and parametric tests were performed. A paired Student's T test with a confidence interval of 95% was conducted to make comparisons of the pre and trans-treatment tipping per tooth and per group (central, lateral, canines, premolars). A one-sample T test was used to compare the values obtained per group with the values of each prescription (MBT and Roth). The data were collected and captured in 2.0 version SPSS for its analysis.
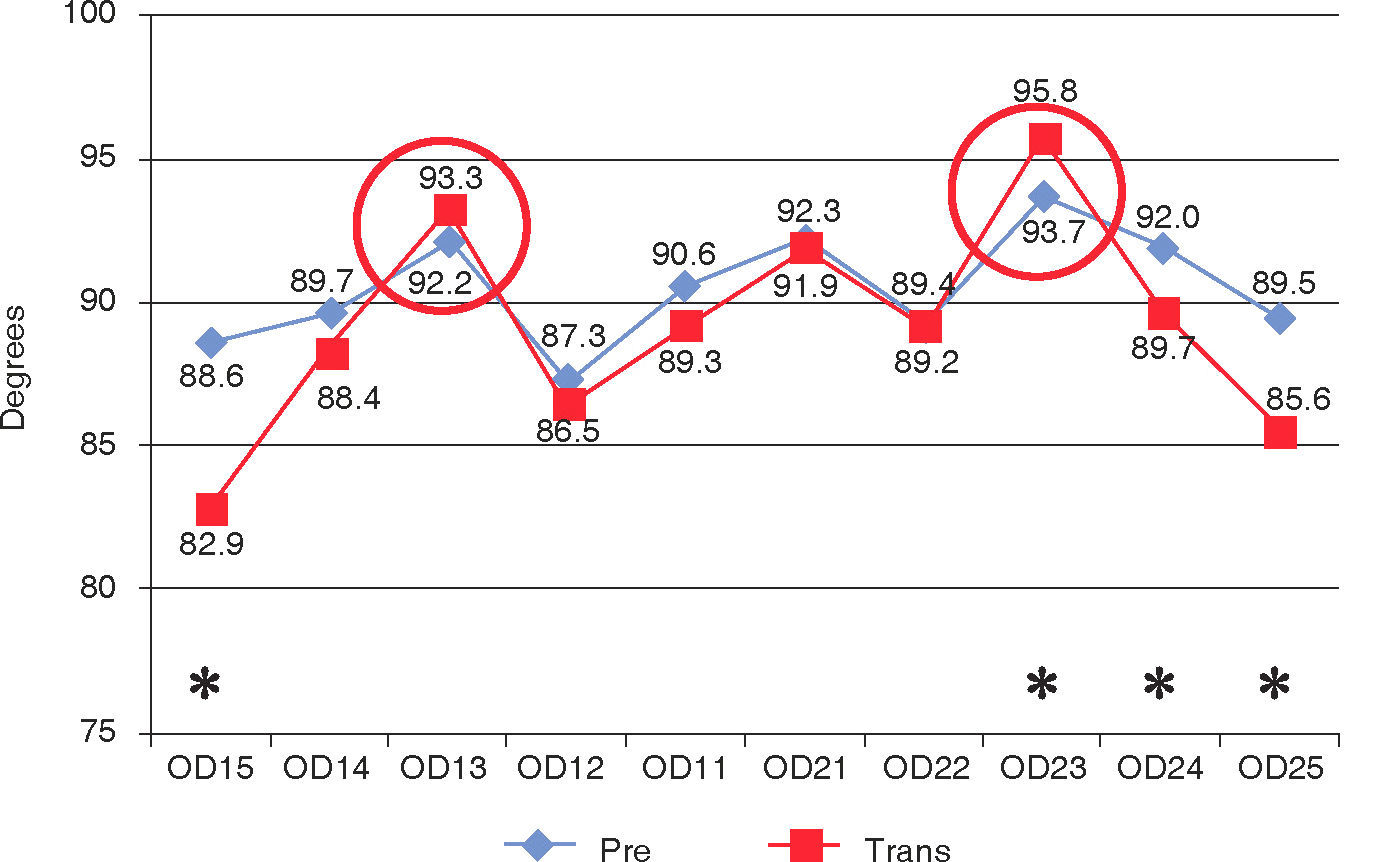
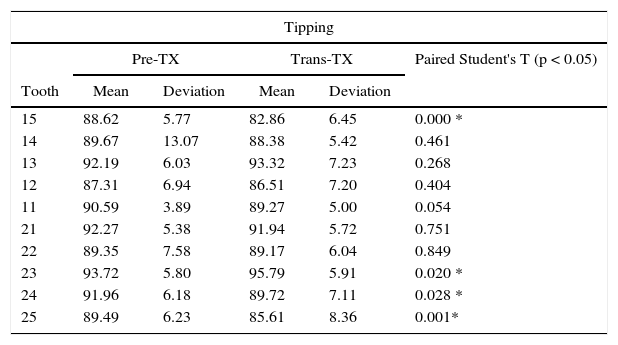
RESULTSRegarding the comparison of the means obtained for the expression of pre and trans-treatment tipping, it was observed that trans-treatment tipping was affected in a negative way; i.e. the distal root inclination decreased unlike the initial or pre-treatment. The canines were the only teeth where trans-treatment tipping was increased or affected in a positive way, as expected according to what is established by the prescriptions. However only statistically significant differences were found in the teeth #15, 23, 24 and 25 (Table II).
Pre and trans-treatment tipping. The asterisk identifies the teeth where statistically significant differences were found.
| Tipping | |||||
|---|---|---|---|---|---|
| Pre-TX | Trans-TX | Paired Student's T (p < 0.05) | |||
| Tooth | Mean | Deviation | Mean | Deviation | |
| 15 | 88.62 | 5.77 | 82.86 | 6.45 | 0.000 * |
| 14 | 89.67 | 13.07 | 88.38 | 5.42 | 0.461 |
| 13 | 92.19 | 6.03 | 93.32 | 7.23 | 0.268 |
| 12 | 87.31 | 6.94 | 86.51 | 7.20 | 0.404 |
| 11 | 90.59 | 3.89 | 89.27 | 5.00 | 0.054 |
| 21 | 92.27 | 5.38 | 91.94 | 5.72 | 0.751 |
| 22 | 89.35 | 7.58 | 89.17 | 6.04 | 0.849 |
| 23 | 93.72 | 5.80 | 95.79 | 5.91 | 0.020 * |
| 24 | 91.96 | 6.18 | 89.72 | 7.11 | 0.028 * |
| 25 | 89.49 | 6.23 | 85.61 | 8.36 | 0.001* |
The asterisk indicates teeth in which significant statistical differences were found.
The posterior segment was the one affected in a negative way, mainly the left side (teeth #24 and 25); the teeth that show the most negative change in transtreatment tipping are the #15 and 25, with differences between 4-6°. Despite the fact that the canines are the only ones that changed in a positive direction with regard to the expression of the trans-treatment tipping, the upper left canine (#23) was the only canine that showed statistically significant differences; while the teeth that maintained the same root distal inclinations were the incisors (Figure 2).

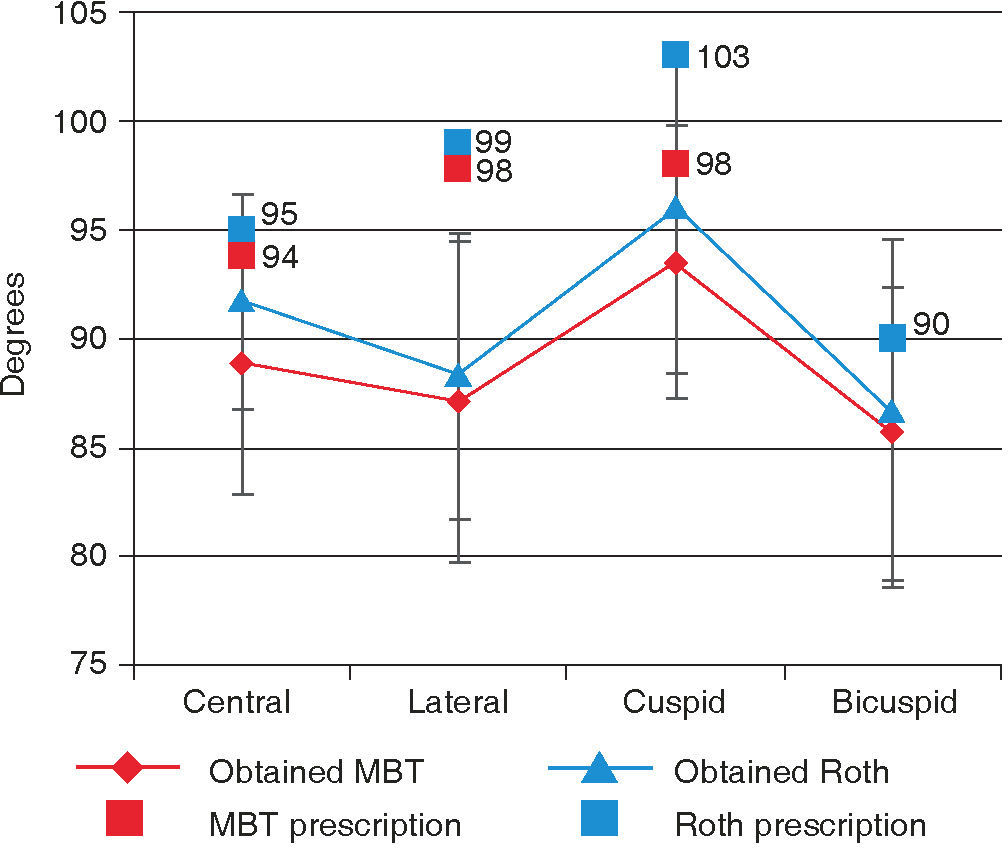
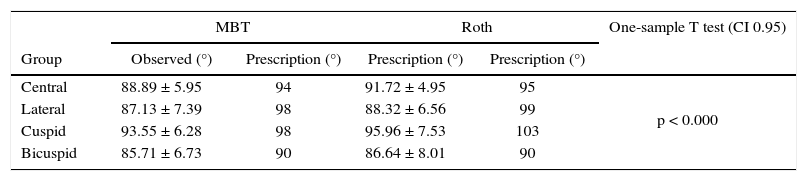
Teeth were classified by group and by orthodontic technique (MBT and Roth), to compare the transtreatment tipping against each prescription. It was observed that in no case the predetermined value was obtained, with differences of 4-6° for central incisors and premolars, and 8-11° for canines and lateral incisors (Table III). Statistically significant differences were found in all groups with both techniques (one-sample t p > 0.05).
Values of trans-treatment tipping compared with those of each prescription (MBT and Roth). Statistically significant differences were found in all groups.
| MBT | Roth | One-sample T test (CI 0.95) | |||
|---|---|---|---|---|---|
| Group | Observed (°) | Prescription (°) | Prescription (°) | Prescription (°) | |
| Central | 88.89 ± 5.95 | 94 | 91.72 ± 4.95 | 95 | p < 0.000 |
| Lateral | 87.13 ± 7.39 | 98 | 88.32 ± 6.56 | 99 | |
| Cuspid | 93.55 ± 6.28 | 98 | 95.96 ± 7.53 | 103 | |
| Bicuspid | 85.71 ± 6.73 | 90 | 86.64 ± 8.01 | 90 | |
Figure 3 presents the values of trans-treatment tipping and those established for each technique. It was observed that despite the fact that the cuspids presented a positive increase, the values established by the respective prescription were not obtained.
DISCUSSION
The results obtained in this investigation are consistent with the studies of Armstrong and Pea8 and Fukuyo5 in stating that bonding error is present regardless of the technique. No matter which orthodontic technique (MBT or Roth) was used, it was observed that the preset values established by the prescription were not obtained in any of the cases thus indicating that despite all the technological advances and improvements in preadjusted appliances, bonding error still persists. This happens as a result of multifactorial aspects; one of the most important is that manufacturing companies prioritize appliance production leaving aside the biological aspect. The diverse prescriptions focus their attention in bracket placement in the clinical crown not contemplating the tooth as a crown-root unit and its surrounding structures (root length, alveolar bone, cortical limits, facial biotype, balance of muscular forces, anatomical abnormalities, among others).
In this study it was observed that the posterior segment on both the right and left sides was negatively affected in terms of trans-treatment tipping expression; this observation is consistent with what was reported by Eliades4 and Suarez;13 since premolars are the teeth that have more anatomical variations, both in convexity of the labial surface as well as in marginal crests level. This same behavior was observed in the left posterior segment, which presented the most negative alteration; mainly because of the visual difficulty that the clinician has when bonding directly. As Joiner9 reported indirect bonding has more precision and entails less clinical time for appliance placement, unlike direct bonding, which was the technique used in this research's sample.
Studies like the one conducted by Moesi et al6 and Israel et al,12 conclude that regardless of the prescription used bonding errors continue to happen, so that it is recognized as a product of human error or lack of skill from the operator. This aspect is important because the sample for this study was taken from patients treated by residents of the Orthodontics specialty. It may be possible that if the sample was taken from patients treated by experienced orthodontists the results would be less dispersed and closer to the values of each prescription. However the results reported by the study of Moesi et al6 show that they found no advantage when comparing MBT and Roth prescriptions on the subjective aesthetic assessment of the completed cases.
CONCLUSIONS- •
Trans-treatment tipping is affected negatively in the posterior sector; the anterior sector is the one that is more stable, while the canines are favored by an increased distal root inclination. In spite of the statements that claim that pre-adjusted appliances optimize the final results of orthodontic treatment, human error or the clinician's ability remains a relevant factor for success with room for improvement and biological issues to consider.
- •
A new bonding technique should be established contemplating the tooth as a crown-root complex and considering its surrounding structures (alveolar bone, root length, cortical limits, facial biotype, balance of muscular forces, anatomical abnormalities, among others), instead of only focusing on the clinical crown as several prescriptions do.