





The case of a patient of 16 years 9 months of age whose chief complaint was «crooked teeth» with skeletal class II, hyperdivergent growth, bilateral molar class I, bilateral canine class II, severe maxillary and mandibular crowding and deviated midlines is hereby reported. The patient did not refer any habit. The treatment consisted in alignment, leveling, detailed and retention with the following appliances: 0.022” x 0.028” Roth prescription brackets. The active treatment time was 1 years 7 months. Thermoformed acetate retainers were placed in the upper and lower arches as well as fixed retainers from teeth #13-23 and 33-43. The treatment was successful obtaining bilateral canine and molar class I, normal overjet and overbite, matching dental midlines, good intercuspation and a harmonic facial profile.
Se reporta un caso de una paciente de 16 años 9 meses, el motivo de consulta fue «tengo los dientes chuecos», es clase II esquelética, hiperdivergente, clase I molar bilateral, clase II canina bilateral, presenta apiñamiento severo maxilar y mandibular, las líneas medias dentales están desviadas. El paciente no refirió ningún hábito. En el tratamiento se realizó una fase ortodóntica que consistió en la alineación, nivelación, detallado y retención con la siguiente aparatología: brackets de autoligado Empower interactivos de prescripción Roth 0.022” x 0.028”. El tiempo de tratamiento activo fue de un año siete meses. Se posicionaron retenedores termoformados superior e inferior y retenedores fijos superior 13- 23 e inferior del 33-43. El resultado del tratamiento fue exitoso, con la obtención de clases I caninas bilaterales, overjet y overbite adecuados, líneas medias coincidentes, correcta intercuspidación y un perfil facial armónico.
In current orthodontic practice, the most commonly used ligation method is elastomeric ligatures, because they facilitate binding the arch wire to the bracket more comfortably for the patient. However, elastomeric ligatures produce more friction than metal ligature.1–3 In response to this fact, new materials that favor the decrease in the sliding resistance (SR), provide greater patient comfort and reduce treatment and chair time have been developed such as self-ligating brackets and low-friction elastomeric ligatures.4–6 The first self-ligating bracket (The Russel Lock) was described by Stolzenberg7 in 1935 but remained practically unnoticed until the 1980's. In these last 39 years approximately 27 new bracket models, or their modifications, have been developed looking for the best option. The desired properties for self-ligating brackets according to Harradine are: safe and resistant; complete filling of the slot by the wire; low friction between wire and bracket; quick and easy to use; allow high friction when necessary; easy placement of elastic strings; facilitate dental hygiene, comfortable for the patient.8 On the other hand, Miles points out that self-ligating brackets have gained popularity due to the fact that their design is characterized by a clip that holds the archwire into the bracket or in some cases, a door that acts as a fourth mobile wall that turns the slot into a tube, which allows the passage of the arch wire on the slot with less sliding resistance.9 However, self-ligating systems have several limitations, such as difficulty to achieve full expression of the prescription of the bracket; the clinical management is sometimes more problematic than with conventional brackets, due to frequent clip failures; brackets are larger and more expensive, and oral hygiene is more difficult due to their complex geometry.2
For these reasons in the last decade low-friction elastomeric ligatures have been introduced to the market. Some of these act as a passive cover on the conventional bracket, allowing the free sliding of the wire in the slot.10 Other low-friction elastomeric ligatures have in their composition an addition of silicone with the aim of reducing the SR. They are highly resistant to pigmentation, very soft and have an excellent stretch and recovery. In addition, consideration should be given to the relationship between the way of placing the elastomeric ligature and the bracket design.10,11
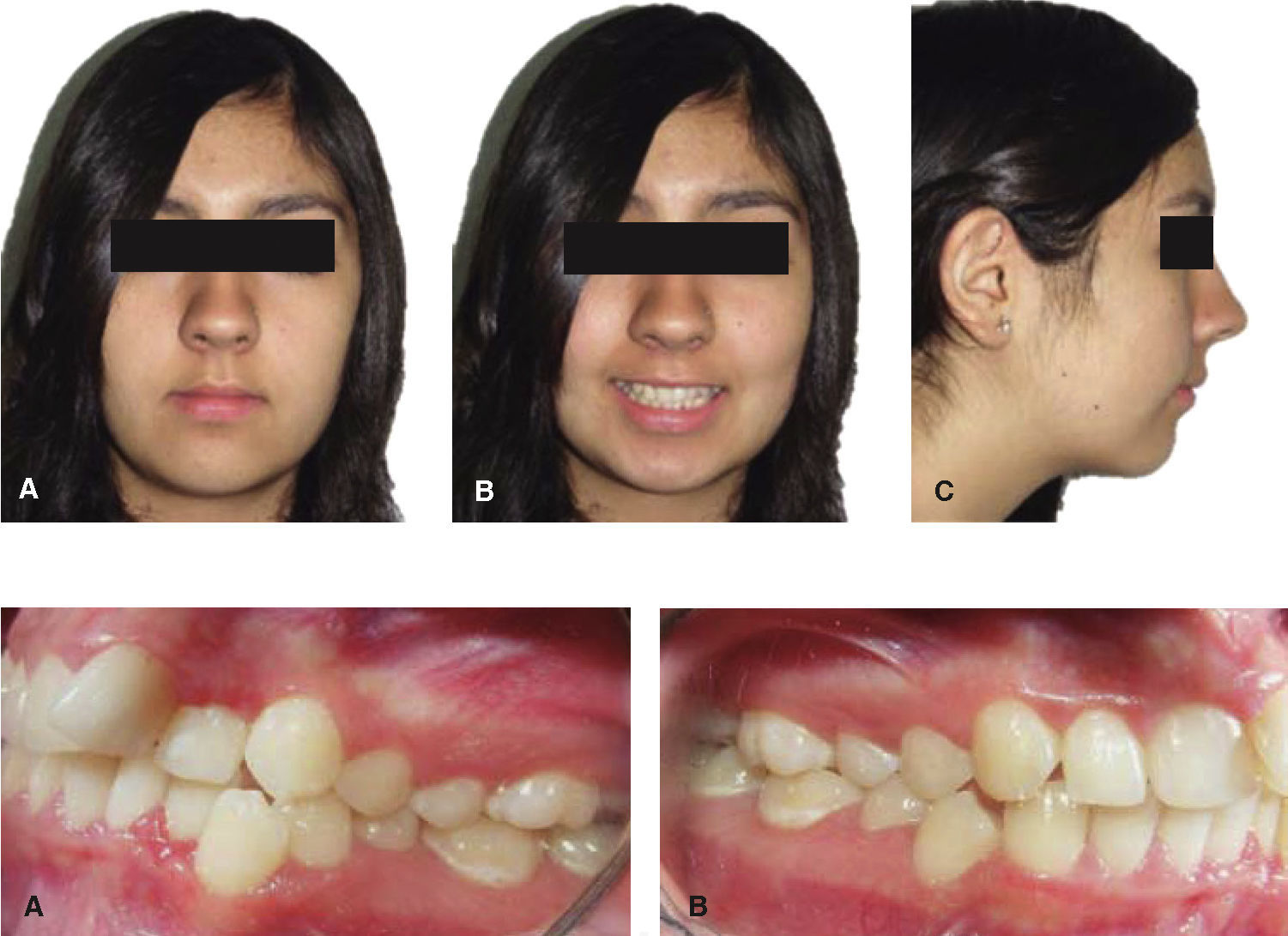
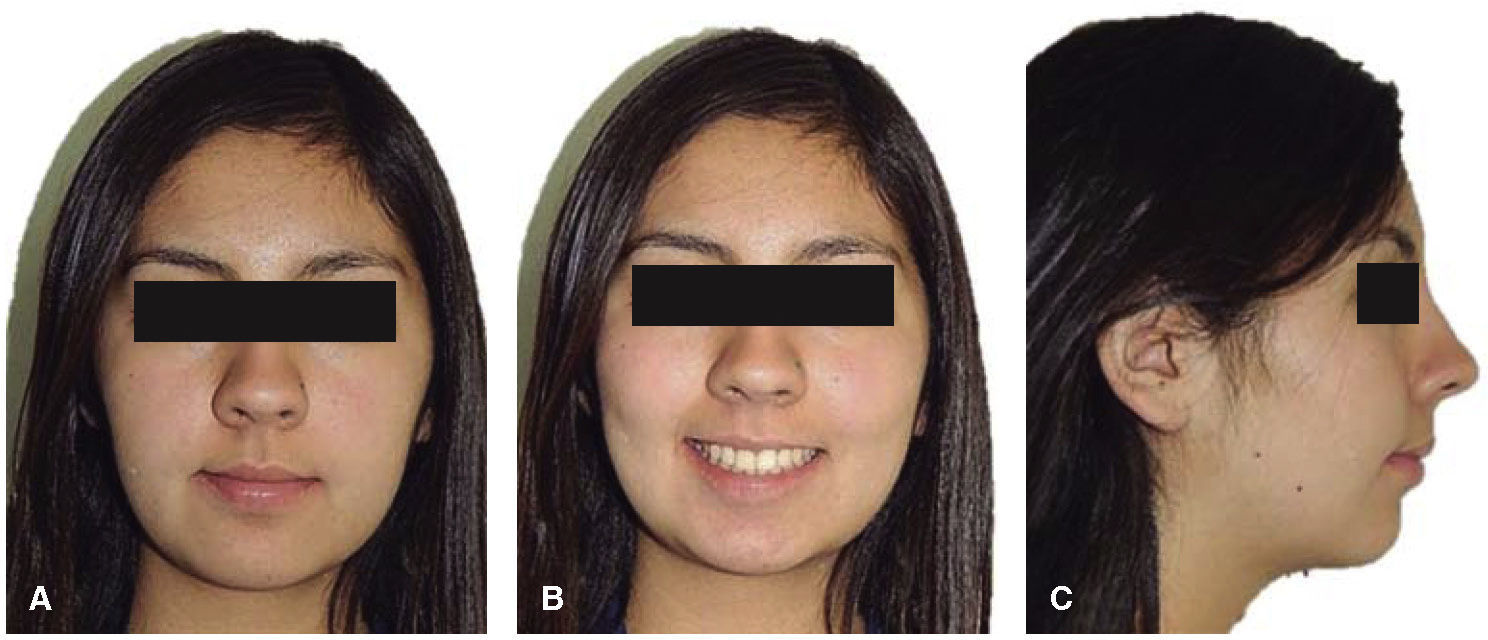
Case report: female patient of 16 years 9 months of age who attended the clinic because she had «crooked teeth». The facial clinical examination, in the frontal photograph (Figure 1A), they are all going in size 10 revealed an apparently symmetrical and dolichofacial patient. In her smile photograph (Figure 1B), the upper dental midline coincides with the facial midline. In the profile photograph (Figure 1C), a convex profile is evident.

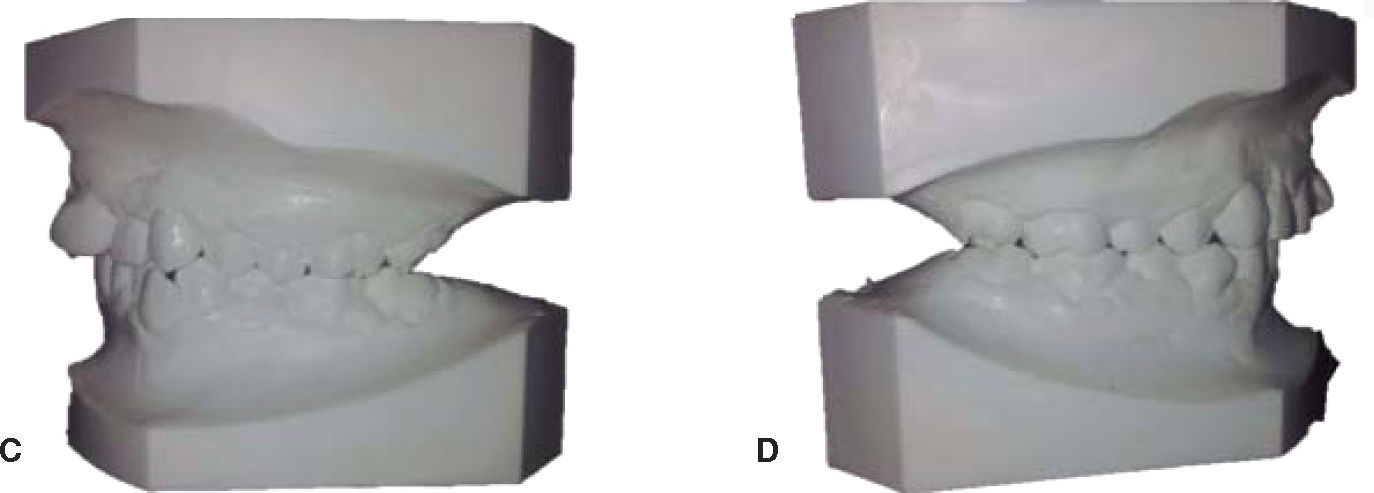
Initial intraoral examination: in the study model analysis and in the initial intraoral photographs, the patient was diagnosed as a bilateral molar class I and canine class II (Figure 2).

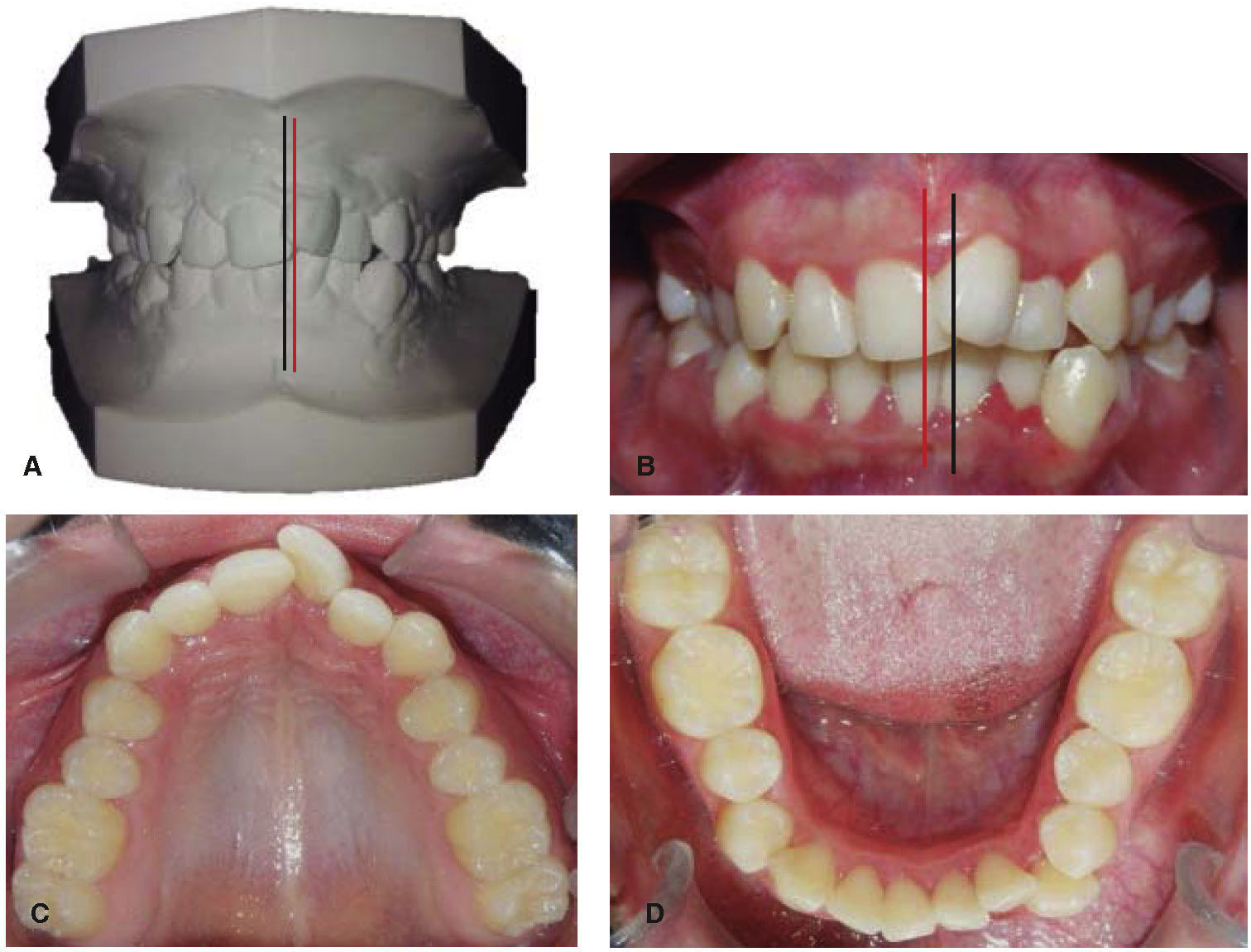
The severe upper and lower crowding was observed as well as the dental midline deviation (Figure 3).

Initial radiographs: the initial lateral headfilm (Figure 4) revealed a skeletal class II, a hyperdivergent growth pattern and abnormal inclinations of the upper and lower incisors.

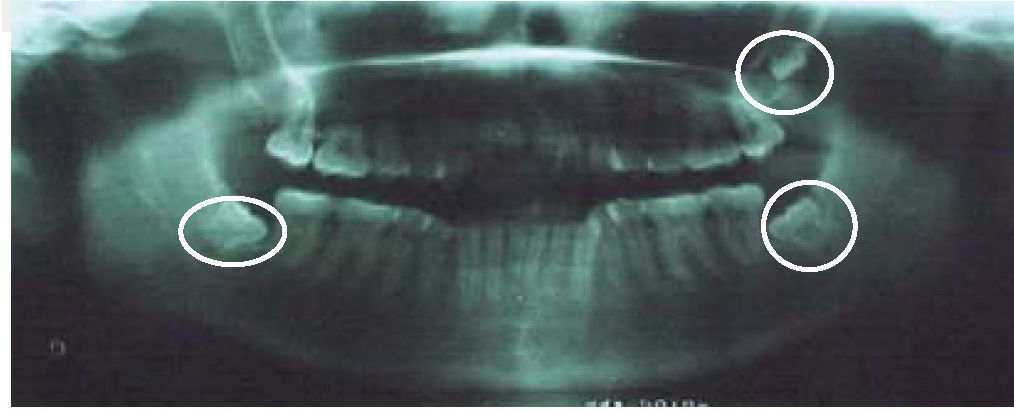
In the initial panoramic radiograph (Figure 5) 31 teeth were observed; the upper and lower third molars were developing.

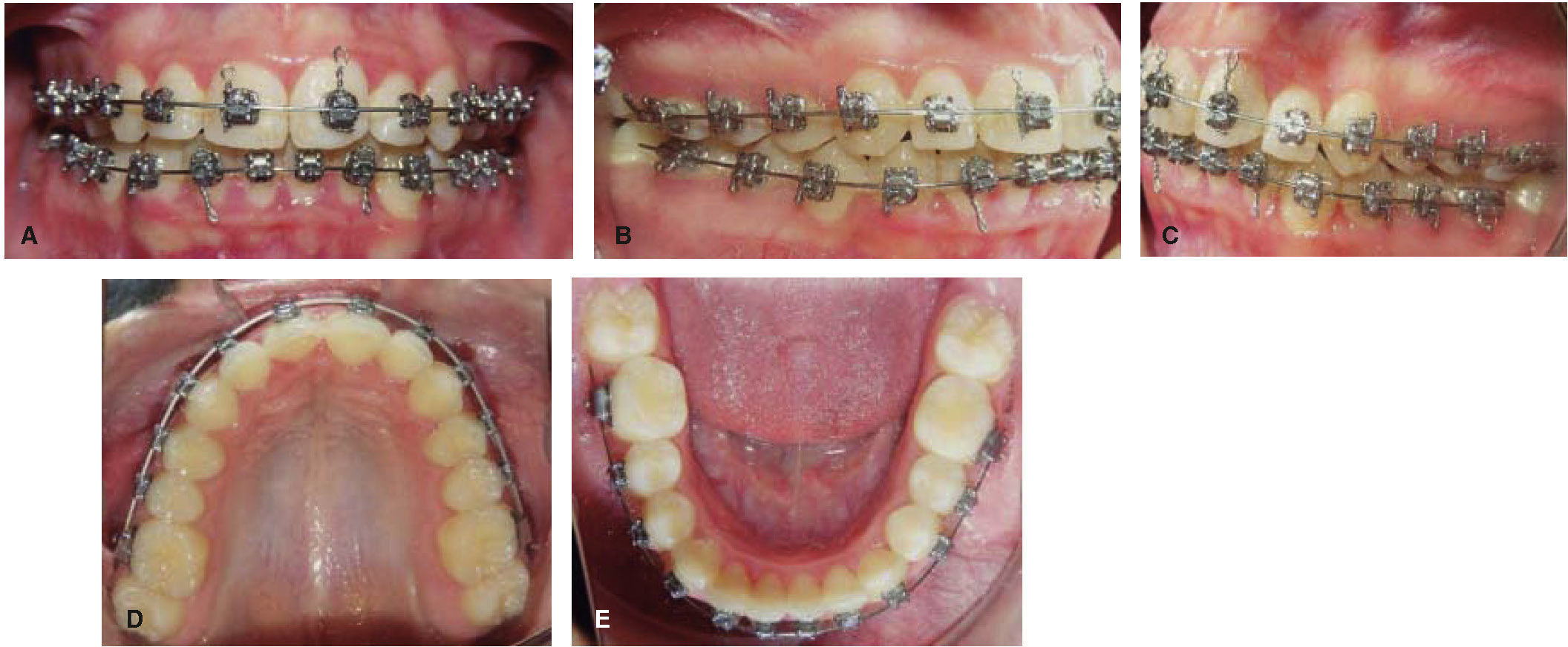
Treatment: treatment consisted of an orthodontic phase with the correction of the maxillary and mandibular crowding through the following sequence of NiTi arch wires: 0.012”, 0.014”, 0.016”, 0.18”, 0.17” x 0.25”; and upper and lower Stainless Steel archwires: 0.020” 0.018”. Leveling, obtaining a normal overjet and overbite, correction of the upper and lower dental midline was performed with stripping and 0.017” x 0.025” stainless steel archwires, intramaxillary chains and class II elastics. Detailing was achieved with anterior box elastics and with first and third order bends. In figures 14 to 18 part of the mechanics that was used during the treatment may be observed.

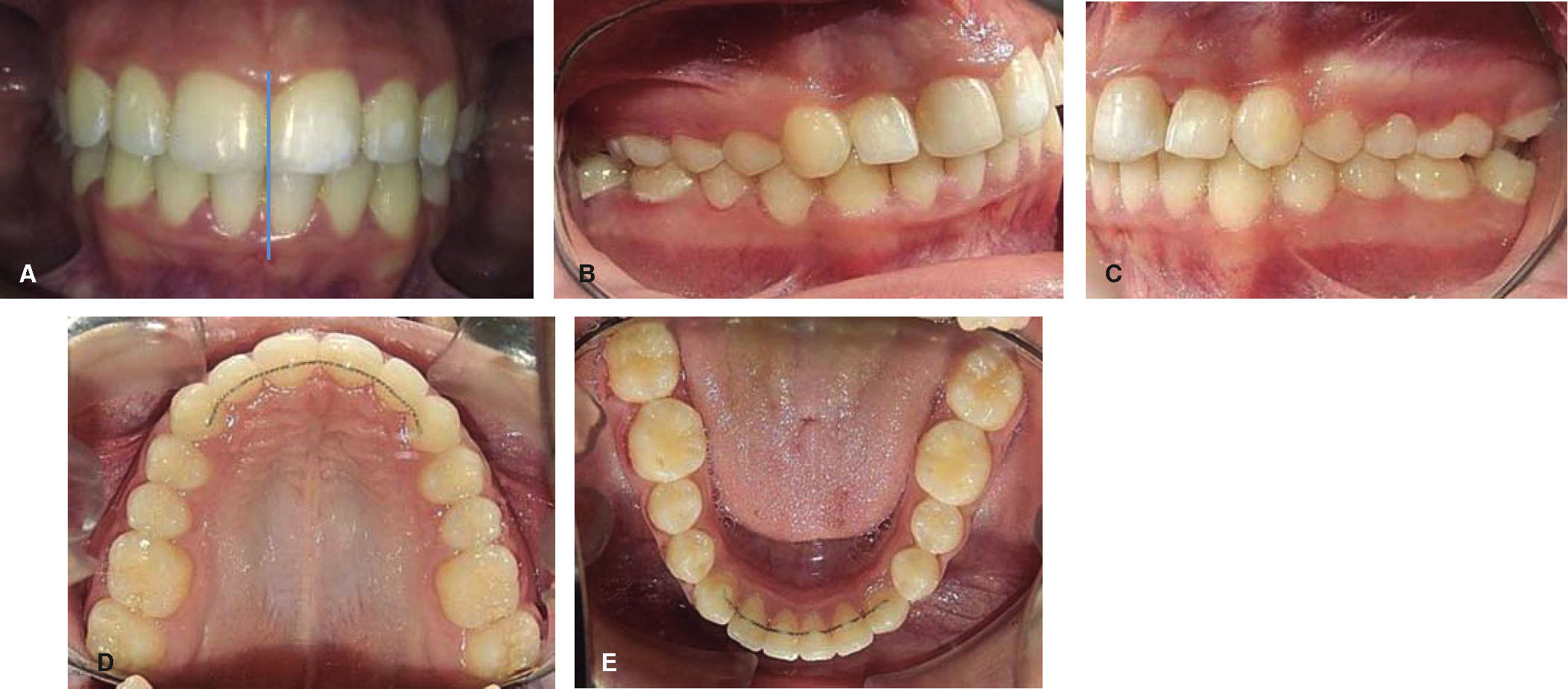
Final studies, 1 year 7 months after initiating treatment a facial clinical examination was performed which showed a good facial balance and profile, facial symmetry, with a broad smile (Figure 7). In the intraoral photographs, the results of treatment may be observed: it was possible to obtain class I molar and canine relationship as well as a normal overjet and overbite (Figure 8).


Intraoral analysis: an adequate overbite, alignment and leveling may be observed as well as coincident dental midlines in (Figure 8A).
Intraoral analysis: in the right and left view (Figures 8A-B) the canine and molar relationships may be noted as well as the final intercuspation and the correction of the severe maxillary and mandibular crowding (Figures 8B-E).
RESULTSThe treatment goals were satisfactorily met, correcting the severe maxillary and mandibular crowding that the patient presented through the use of Empower interactive self-ligating brackets. The final lateral headfilm (Figure 9) shows a skeletal class II relationship, the patient's hyperdivergency and correct inclinations of the upper and lower incisors. The patient at the end of orthodontic treatment presented a suitable facial profile, the severe maxillary and mandibular crowding was resolved and bilateral canine class I and molar class I was achieved. The dental midlines matched, the overjet and overbite were normal; there was good root parallelism as well as canine and incisive guidance.

In the final panoramic radiograph 29 teeth were present; the lower third molars were extracted (Figure 10). For retention and stability of treatment in addition to preserving intercanine width, thermoformed retainers were placed in both the upper and the lower arches as well as fixed retainers from canine to canine.
DISCUSSION
Shivapuja and Berger12 found that self-ligating brackets generate less friction than conventional systems. Hanson13 found similar results and concluded that this could reduce treatment time. Voudouris14 found that self-ligating brackets, whether passive or active, produce less friction than conventional brackets with ligature wire. However, Read Ward et al,15 found that self-ligating brackets produce less friction only under certain conditions. In the case hereby presented, optimum results were achieved with Empower interactive self-ligating brackets that generate less friction than conventional systems thus solving the severe maxillary and mandibular crowding. With regard to treatment time, it was equal to the average time of orthodontic treatment with conventional systems.
CONCLUSIONSSelf-ligating systems constitute a novel option in orthodontics. The self-ligating system is an orthodontic technique that uses brackets with a gate that holds a stainless steel wire of high quality. When the gate is closed, the wire is held by the bracket, which is bonded to the tooth. Thanks to this union the tooth moves very quickly causing less disruption to the patient during treatment than with a conventional bracket.
Self-ligating brackets may be active or passive. Active self-ligating brackets produce a larger clinically usable torque variation, have better torque control and less play of the wire in the slot than passive selfligating brackets.