


La fisiología tiroidea sufre cambios adaptativos durante la gestación, haciendo necesario conocer los límites de normalidad de las hormonas tiroideas según la edad gestacional para una correcta interpretación, principalmente en la enfermedad tiroidea subclínica. Los sistemas de información de laboratorio (SIL) encuentran dificultades para informar rangos de referencia ante diferentes situaciones fisiopatológicas. La labor del facultativo del laboratorio es importante para desarrollar y diseñar herramientas que permitan identificar estas situaciones e interpretar los resultados de forma adecuada.
ObjetivoAnalizar si el cambio del SIL en nuestro servicio y la emisión del informe del laboratorio con la interpretación de los resultados, habían tenido repercusión sobre la identificación y el seguimiento de la disfunción tiroidea en las gestantes de nuestra área.
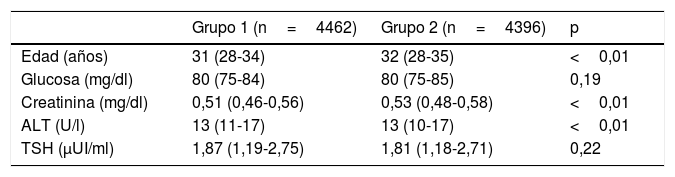
Material y métodosSe ha realizado un estudio retrospectivo transversal analizando los resultados de las analíticas de todas las gestantes de primer trimestre y a las que se les habían solicitado pruebas tiroideas en los siguientes 6 meses. Se realizaron 2 grupos, antes y después del cambio de SIL.
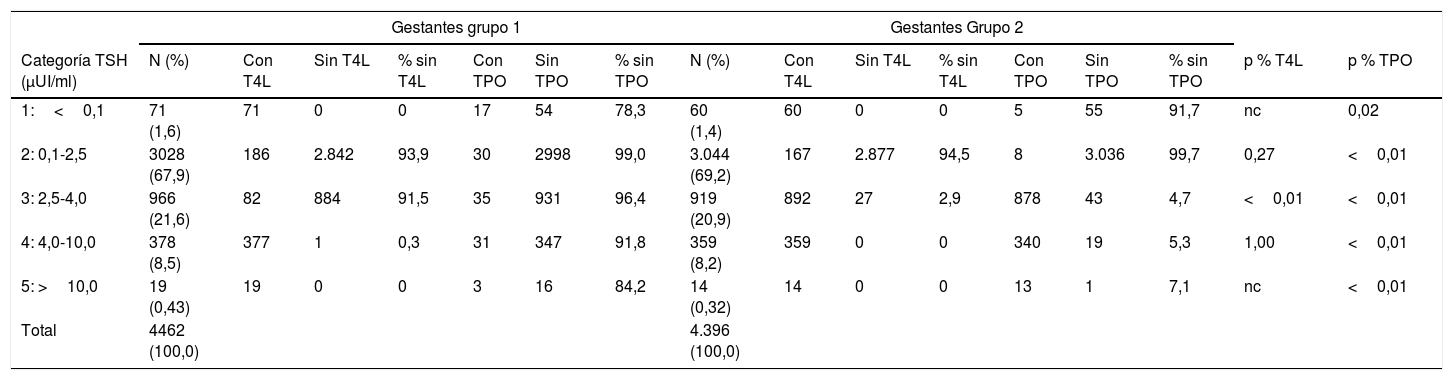
ResultadosLos porcentajes de seguimiento fueron similares en los 2 grupos, excepto cuando la TSH era patológica para gestantes y normal para población general, es decir, cuando no salía asterisco.
ConclusionesLos rangos de referencia establecidos para población normal no identifican la enfermedad tiroidea subclínica en gestantes. Es imprescindible la intervención activa del facultativo del laboratorio en la valoración de estos resultados. En nuestro estudio un 50% más de las gestantes con hipotiroidismo subclínico se benefició de la estrategia que habíamos introducido.
Thyroid physiology undergoes adaptive changes during pregnancy, making it necessary to know the reference ranges of thyroid hormones according to gestational age for a correct interpretation, especially in subclinical thyroid disease. Laboratory information systems (LIS) have difficulty in reporting reference ranges (RR) in different pathophysiological situations. The work of the laboratory physician is important in developing and designing tools to identify these situations, and to make an appropriate interpretation of the results.
ObjectiveTo determine whether the change in the LIS in our department and the issue of the laboratory report with the interpretation of the results, had an impact on the identification and monitoring of thyroid dysfunction in pregnant women in our area.
Material and methodsA retrospective cross-sectional study was carried out by analysing the results of all first-trimester pregnant women and those on whom thyroid tests had been requested in the following six months. The pregnant women were divided into two groups, before and after the change of the LIS.
ResultsFollow-up percentages were similar in the two groups, except when TSH was abnormal for pregnant women and normal for the general population, that is, when there was no asterisk.
ConclusionsThe RRs established for the normal population do not identify sub-clinical thyroid disease in pregnant women. The active intervention of the laboratory physician is essential in the evaluation of these results. In our study, more than 50% of the pregnant women with sub-clinical hypothyroidism benefited from the strategy introduced.
Artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
