


Alzheimer's disease has been studied from various areas of knowledge (biomarkers, brain structure, behavior, cognitive impairment). Our aim was to examine the effects of an exercises protocol developed using complexity theory concepts.
MethodExercise improves neuroplasticity (neuronal ability to change and adapt as a result of experience) through mental and physical skills linked to cognitive-associative brain circuits. Introducing controlled physical and cognitive stimuli, self-organization and connectivity among brain systems enhance. We used tasks with non-linear outputs (several solutions) and learning as order parameter. Tasks were performed simultaneously, at the edge of the error seeking self-organized criticality.
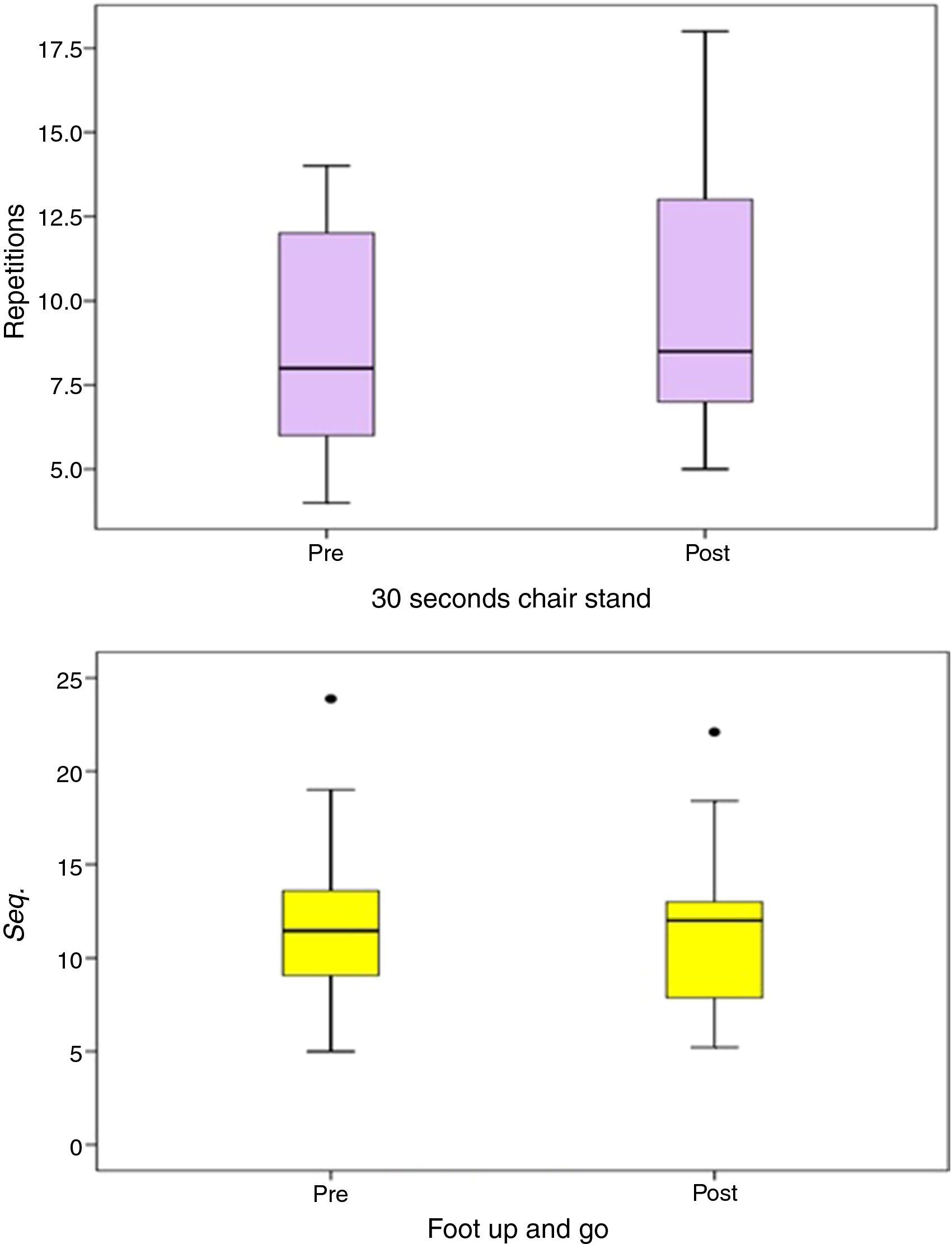
ResultsScreening tests data showed a reduction in cognitive impairment, which suggests a reduction disease progression, in terms of executive function. There was a marked improvement in the physical tests: 30seconds chair stand test (PRE: 8.78±3.46; POST: 9.44±3.68 repetitions) and foot up and go test (PRE: 11.95±5.19; POST: 11.69±4.43seconds).
ConclusionResults showed that patient's self-organization was increased; behaviors atrophied or inhibited reappeared. Using these controlled perturbations, Alzheimer's Disease patients were able to manifest improvements in both their mental and physical abilities.
La enfermedad de Alzheimer ha sido estudiada desde varias áreas del conocimiento (biomarcadores, estructura cerebral, conducta, discapacidad cognitiva). Nuestro objetivo ha sido examinar de un protocolo de ejercicio diseñado usando conceptos de la teoría de los sistemas complejos.
MétodoEl ejercicio mejora la neuroplasticidad (habilidad neuronal para el cambio y adaptación como resultado de la experiencia) a través de las habilidades mentales y físicas vinculadas a los circuitos cerebrales cognitivo-asociativos. La inclusión de estímulos físicos y cognitivos controlados mejora la autoorganización y la conectividad entre los sistemas cerebrales. Hemos utilizado tareas con soluciones no lineales (varias soluciones) y hemos analizado el aprendizaje. Las tareas se realizaron simultáneamente en el límite del error buscando la autoorganización crítica.
ResultadosEl análisis de nuestros datos mostró una reducción del deterioro cognitivo, lo que sugiere un enlentecimiento de la progresión de la enfermedad, en términos de la función ejecutiva. Se constató una marcada mejoría en las pruebas físicas: Test de sentarse y levantarse durante 30′ (PRE: 8.78±3.46; POST: 9.44±3.68 repeticiones) y Test de levantarse y caminar (PRE: 11.95±5.19; POST: 11.69±4.43 segundos).
ConclusiónLos resultados mostraron que la autoorganización del paciente mejoró y que reaparecieron conductas atrofiadas o inhibidas. Utilizando estos estímulos controlados, los pacientes con Alzheimer fueron capaces de manifestar mejoras en sus capacidades mentales y físicas.
A doença de Alzheimer tem sido estudada por várias áreas do conhecimento (biomarcadores, estrutura cerebral, comportamento, déficit cognitivo). Nosso objetivo foi examinar os efeitos de um protocolo de exercícios desenvolvidos com os conceitos da teoria da complexidade.
MétodoO exercício melhora a neuroplasticidade (a capacidade neural para mudar e adaptar-se, como resultado de experiências) através de habilidades mentais e físicas ligadas a circuitos cerebrais cognitivo-associativos. Apresentando estímulos físicos e cognitivos controladas; auto-organização e aumento da conectividade entre os sistemas cerebrais. Usamos tarefas com saídas não-lineares (várias soluções) e de aprendizagem como parâmetro de ordem. As tarefas foram realizadas em simultâneo, no limite do erro em busca da criticalidade auto-organizada.
ResultadosAs triagens de dados testes mostraram uma redução no déficit cognitivo, o que sugere redução na progressão da doença, em termos de função executiva. Houve uma melhora acentuada nos testes físicos: 30 segundos no testes sentar e levantar da cadeira (PRE: 8.78±3.46; POST: 9.44±3.68 repetições) e no teste de levantar e caminhar (PRE: 11.95±5.19; POST: 11.69±4.43 segundos).
ConclusõesOs resultados mostraram que a auto-organização do paciente foi aumentada; reapareceu comportamentos atrofiados ou inibidos. Usando estas perturbações controladas, os pacientes com doença de Alzheimer foram capazes de manifestar melhorias em suas capacidades físicas e mentais.
The Alzheimer's Disease (AD) is a neurodegenerative disease characterized by or accumulation of proteins such as Tau or β-amyloid, which causes progressive dementia in adulthood, leading to a state of total disability and death.1,2 AD currently affects in Spain about 600000 people (25% of those over 65 years) and about 44 million people worldwide. It is the most common cause of dementia in Europe and perhaps the most common neurodegenerative disease worldwide. The costs of caring for people with this disease in Spain amounted to 37000 million euros annually.
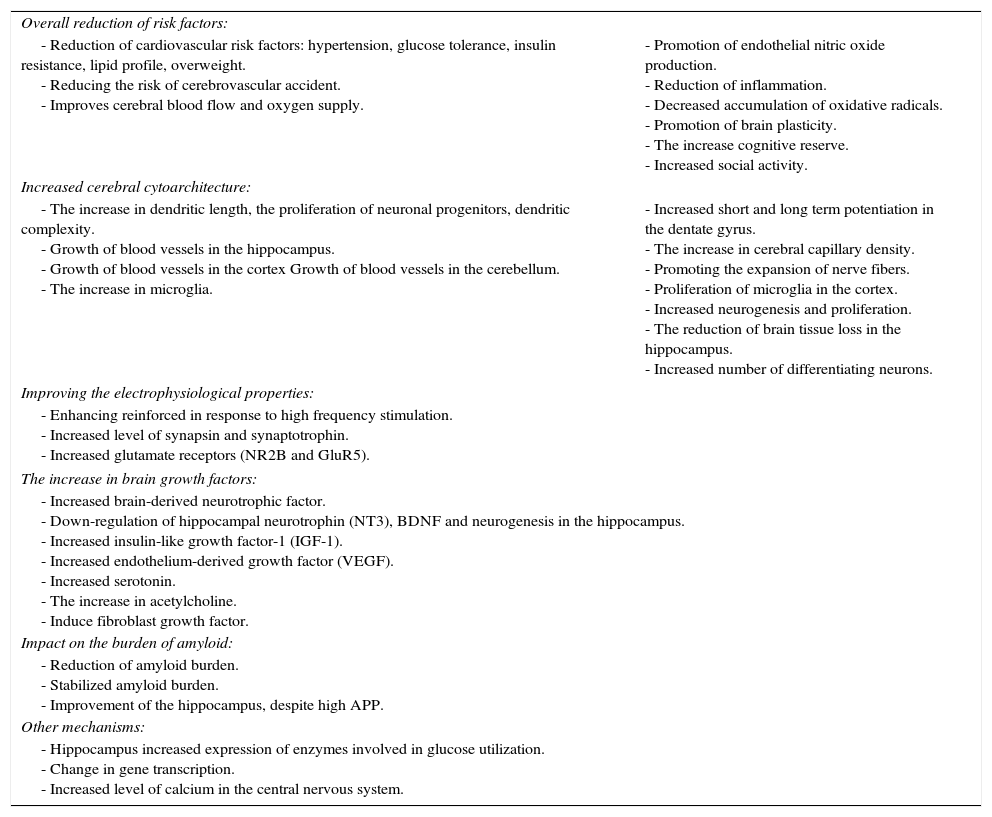
Exercise has previously been proven to have a positive effect on AD patients. Exercise can increase levels of brain-derived neurotrophic factor (BDNF) and other growth factors, stimulate neurogenesis, increase resistance to brain injury, improve learning and mental performance, arouse the growth of blood vessels, reduce of amyloid load, etc. (Table 1).3–6 But the point is what kind of training?
Main benefits of the physical activity on Alzheimer's disease (extracted from6).
| Overall reduction of risk factors: | |
| - Reduction of cardiovascular risk factors: hypertension, glucose tolerance, insulin resistance, lipid profile, overweight. - Reducing the risk of cerebrovascular accident. - Improves cerebral blood flow and oxygen supply. | - Promotion of endothelial nitric oxide production. - Reduction of inflammation. - Decreased accumulation of oxidative radicals. - Promotion of brain plasticity. - The increase cognitive reserve. - Increased social activity. |
| Increased cerebral cytoarchitecture: | |
| - The increase in dendritic length, the proliferation of neuronal progenitors, dendritic complexity. - Growth of blood vessels in the hippocampus. - Growth of blood vessels in the cortex Growth of blood vessels in the cerebellum. - The increase in microglia. | - Increased short and long term potentiation in the dentate gyrus. - The increase in cerebral capillary density. - Promoting the expansion of nerve fibers. - Proliferation of microglia in the cortex. - Increased neurogenesis and proliferation. - The reduction of brain tissue loss in the hippocampus. - Increased number of differentiating neurons. |
| Improving the electrophysiological properties: | |
| - Enhancing reinforced in response to high frequency stimulation. - Increased level of synapsin and synaptotrophin. - Increased glutamate receptors (NR2B and GluR5). | |
| The increase in brain growth factors: | |
| - Increased brain-derived neurotrophic factor. - Down-regulation of hippocampal neurotrophin (NT3), BDNF and neurogenesis in the hippocampus. - Increased insulin-like growth factor-1 (IGF-1). - Increased endothelium-derived growth factor (VEGF). - Increased serotonin. - The increase in acetylcholine. - Induce fibroblast growth factor. | |
| Impact on the burden of amyloid: | |
| - Reduction of amyloid burden. - Stabilized amyloid burden. - Improvement of the hippocampus, despite high APP. | |
| Other mechanisms: | |
| - Hippocampus increased expression of enzymes involved in glucose utilization. - Change in gene transcription. - Increased level of calcium in the central nervous system. | |
Most authors focus on exercises for improving the manifestations of physical fitness in isolation way, and as an indirect result, seek to reduce the advance of the disease. In our opinion, this is an error because nature does not work in that way. There is not a separation between body and mind. All levels, in body and nature, are connected and influence each other. Sport reality shows us that in its different levels (including brain), structure, shape and functionality evolve in time and are closely related to performance.7–14 This is the result of an evolutionary process through nonlinear interactions in many biological and non-biological systems.15–20
Consequently, and following the asseveration: “I am I and my circumstance”,21 it is not possible to understand the reality of an individual by isolating of the relationships with his own universe. Interaction means cooperation-opposition among individual systems and environment (physical and social). In fact, a long-standing problem in biological and social sciences is to understand the conditions required for the emergence and maintenance of cooperation in evolving populations.22,23 Ergo the key strategy we propose is the interaction of well-defined units in order to promote cooperation among body systems, to promote self-organization. That is why we applied the concept of Holistic Training (body systems synergy: The whole is greater than the sum of its parts) in order to develop a training program for AD. This is a very interesting tool due to the availability, low cost, no invasiveness and improvement of comorbidities associated with aging.
The concept of self-organization can be expressed as the general tendency of a given system to generate behavior patterns from local interactions of its constituent elements and the relationships with the environment.8,24–27 This phenomenon enables people to develop sport skills, resolve mental challenges, assimilate training loads and improve, keep body temperature, repair wounds, etc. According to Goodwin, if want to improve the system, the ideal is to investigate the conditions that promote self-organization.28 It is true that if we review the literature about exercise and AD, we can observe that there are not clear methodologies to deal with AD patients. Perhaps this may be because the sources causes of patients crisis and conditions associated with AD (depression, stress, etc.) are different in each case and display different outputs to the same stimulus. This does not allow generalize as in other study populations.
MethodSubjectsUsing complexity theory concepts, we carried out an intervention program in order to diminish the deterioration of cognitive and motor functions with a sample of 18 moderate grade Alzheimer's Disease patients (12 women; 6 men, 75.78±5.53 years; body weight: 64.19±13.15kg; height: 1.57±0.08m. Body Mass Index (BMI): 25.84±4.28kg/m2). The original sample was bigger but we excluded those who did not complete all training sessions. The sample belonged to a group of subjects of Canary Alzheimer Association, who voluntarily participated in the investigation. Patient's relatives and the Director of Canary Alzheimer Association were informed of the characteristics of the study and signed a written consent. All study participants rigorously followed the criteria proposed in the Declaration of Helsinki for research involving human subjects.
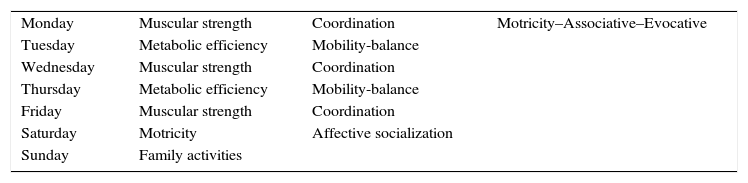
Experimental proceduresThe intervention program for this study was conducted in small groups of two people per coach, during 16 weeks with a frequency of five sessions per week and 60minutes per session. We designed a circuit of stations where the subjects performed exercises of various guidelines aimed to develop balance, joint mobility, coordination, muscular strength and metabolic efficiency with the following protocol (Table 2). Physical, mental, and evocation tasks were performed simultaneously:
- -
Coordination: tasks involving fine motor manipulations: throwing and receiving of objects (one and two hands), manipulating objects and use of implements; and variants of these exercises.
- -
Balance: tasks that involve improving the static and dynamic balance, balance shaft bipodal hip displacement (oscillations), bipodal balance by manipulation, changing the method of balancing. Unipodal balance, unipodal balance with manipulation. Movements in different directions and rhythms (open and close eyes); travel with address changes and rhythms, movements directed and conditioned. And similar exercises for the same purpose.
- -
Mobility: tasks that involve improving of motion range of joints of upper and lower limbs. Stretching the muscles that affect the ankle, knee and hip. Stretching the muscles that affects the joints of the wrist, elbow and shoulder.
- -
Endurance (metabolic efficiency): aerobic loads of low-impact and intensity at reclining cycloergometer adding fine motor and cooperatives tasks.
- -
Strength (muscle tone): directed tasks, primarily, to the lower limb muscles with your own body weight or using external loads on weights machines.
Periodization and orientation training.
| Monday | Muscular strength | Coordination | Motricity–Associative–Evocative |
| Tuesday | Metabolic efficiency | Mobility-balance | |
| Wednesday | Muscular strength | Coordination | |
| Thursday | Metabolic efficiency | Mobility-balance | |
| Friday | Muscular strength | Coordination | |
| Saturday | Motricity | Affective socialization | |
| Sunday | Family activities | ||
Initial training loads were based on motor control: coordinative elements and transfer strength loads adapted to daily life. Recommendations were to guaranteed strength in the entire range movement (no affect integrity of the weak points), use variations of the same exercise, increase the training load density (intensity and volume) and evolved toward harder training loads in order to adapt the body to special motor regime.29
We used regular training equipment such as static bikes, fitballs, benches, ropes, cones, steps, tennis balls, gymnastics balls, medicine balls, elastics bands, hockey sticks, barbells, dumbbells, hurdles, ping-pong paddles, etc., Specific material such us unstable platforms, whole body vibration platform, isoinertial machine, evocation material (photos, music, projections on the wall, etc.).
We designed exercises with non-linear outputs (several solutions) that evolved from great symmetry exercises (less complicated) to lower symmetry exercises (more complicated). Unpredictability is the creative basis of this process. The objective was that introducing controlled physical and cognitive stimuli (perturbations) self-organization among brain systems would enhance. Tasks were developed in parallel to processes of evocation and cognitive association individually designed. Coaches knew the patients’ medical histories, in order to minimize stress on the patients (nervous breakdowns situations caused by a particular subject matter). The increasing rate of task difficulty was determined separately for each patient: when a patient succeeded a certain level of task, he/she was then moved on to a harder level; or vice versa. The relationship between the acquisition of a skill, the speed of task completion, and the number of practice trials is well approximated by a power law.9,30 Therefore, learning acts as an order parameter. If the subject fails too much, a critical point shows up and the Power Law becomes in a truncated Power Law, which points out the rhythm/area where we have to work close to. These processes took place simultaneously and continuously during workout time. Always next to the edge of the error seeking self-organized criticality. Self-organization enhance because a harder task implies higher neuroplasticity.
The cognitive assessment was done by different test of screening: MMSE (Mini-Mental State Examination) with maximum score of 30 points, Cricthon (indicates level of cognitive impairment) with maximum score of 38, STI (Set-Test of Isaacs) of verbal fluency with maximum score of 40, CDT or Clock Drawing Test with a maximum score of 10 points and TMT or Trail Making Test in parts (A/B) which collects the runtime. For the analysis of the data were taken as control variables to study the age, sex and years of schooling of the subjects in the sample.
Statistical analysisFor a description of the study variables of the sample was carried out descriptive statistics of the variables evaluated in the physical test (get up and sit, stand and walk) and cognitive [MMSE, CRICHTON, STI, CDT, TMT (A/B)].
After a normality analysis Shapiro–Wilk of the variables, we carried out a mean comparison between the results of the Pre-Intervention and the Post-Intervention for paired samples. A T-test calculation was used for comparison of means related parametric and T-Wilcoxon for comparison of means related nonparametric. The decision statistics were calculated by taking a level of significance p<0.05.
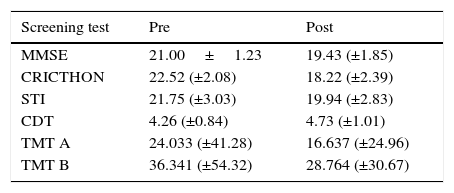
ResultsThe MMSE, STI, CDT and TMT-A screening tests data showed no significant differences (see Table 3), while the CRICHTON and TMT-B showed statistically significant differences (p=0.022; p=0.018). There was a moderate reduction in cognitive impairment, which suggests a slowed disease progression, at least in terms of executive function. There was a remarkable decrease in TMT-A execution time (TE=0.31s). TMT-B shows statistically significant differences (p<0.05) in regards to the achievement of the test time (time conditioned by the execution).
Pre- and post-intervention screening test results.
| Screening test | Pre | Post |
|---|---|---|
| MMSE | 21.00±1.23 | 19.43 (±1.85) |
| CRICTHON | 22.52 (±2.08) | 18.22 (±2.39) |
| STI | 21.75 (±3.03) | 19.94 (±2.83) |
| CDT | 4.26 (±0.84) | 4.73 (±1.01) |
| TMT A | 24.033 (±41.28) | 16.637 (±24.96) |
| TMT B | 36.341 (±54.32) | 28.764 (±30.67) |
Pre: pre intervention; Post: post intervention; MMSE: Mini-Mental State Examination; Cricthon: level of cognitive impairment; STI: Set-Test of Isaacs; CDT: Clock Drawing Test; TMT A: Trail Making Test parts A; TMT B: Trail Making Test parts B.
There was a marked improvement in the 30seconds chair stand test (see Fig. 1). Repetitions increased by 7.1% (PRE: 8.78±3.46; POST: 9.44±3.68 repetitions). In the foot up and go test, the time to get up, cover the distance (2.45m), and sit down, decreased slightly (2.2%) (PRE: 11.95±5.19; POST: 11.69±4.43seconds).
Discussion and foot up and go (below) tests.")
The results show that patient's self-organization was increased and behaviors that had atrophied or inhibited tended to reappear, which can be understood as an emergency.31–34 New properties emerged due to these controlled perturbations, which stimulate self-organization.32,35,36 These perturbations produce bifurcations involving order parameter in terms of learning rates, which some authors describe by several equations.32
Furthermore, in the beginning of the program, the subjects were unable to carry out the motor and cognitive tasks simultaneously. They stopped the movement and then answered the questions. Their systems were not synchronized. But after a while, with training, they were able to resolve the tasks simultaneously. Self-organization, that provides an example on a human scale of the synchronization processes that occur in numerous natural systems, finally appeared. Néda37 give us a beautiful example of how initially, the clapping of the audience is non-synchronized, but after a while they settles down in a common rhythmic and synchronized clapping pattern.
In fact, one of the keys to our success was to establish appropriate working groups. We selected the couples with more affinity, able to help each other and to produce a pleasant sensation for the workmate. Unconsciously, our minds are connected. We create networks with people nearby through mirror neurons.38 These mechanisms encourage the processes of our mental networks, and with adequate training mental (stimulation) synchronization processes are positively enhanced. Perception plays an important role, because is a bipolar process (cognitive-sensorial).39 According to James39 one part of what we perceive comes through the senses, what we have in front of us. And another part always comes from our own mind. Hence it is called bipolar process because of this dual side: sensory and cognitive. Perception depends on the individual and personal characteristics of each subject. It depends on stimuli and sensory organs. In short, it depends on the activity of perceiving subject and perceptual schemas. In perception are involved learning, past experiences, cultural, motivations, expectations, skills, personality, habits and memories. Perception is an active process. All influence on the selection and interpretation of data and content. Therefore, our training has taken a multidimensional approach. Information flow is generated by the constituent elements that in turn changes the status of the source,40 because interactions between units in systems usually give rise to intricate networks with non-trivial structure, which affects the dynamics and properties of the system.41
Our findings suggest that AD patients who trained using concepts from complexity theory may be able to manifest improvements in both their mental and physical abilities. They showed a slight tendency of stabilization or a slowing of cognitive impairment aspects assessed in the MMSE, Crichton, STI and CDT; and a clear improvement of executive procedures by reducing the execution time of part A and B of the TMT.
Conflict of interestThe authors have no conflicts of interest to declare.
We want to give thanks to the Canary Alzheimer Association Staff and the families.
