


Papillary fibroelastomas are rare benign primary cardiac tumors that usually grow depending on the left heart valves. The pulmonary valve is rarely involved, with only 7% of cases described on it. Most of patients are asymptomatic but these tumors are responsible for life-threatening complications. We present a singular case of papillary fibroelastoma depending on the pulmonary valve in a young woman detected by echocardiography which was surgically removed with an uneventful recovery.
Los fibroelastomas papilares son unos tumores cardíacos primarios que normalmente crecen dependiendo de las válvulas cardíacas izquierdas. La válvula pulmonar rara vez se ve involucrada, estando presente en tan solo un 7% de los casos descritos. La mayoría de los pacientes están asintomáticos, pero estos tumores son responsables de las complicaciones potencialmente mortales. Se presenta un caso singular de fibroelastoma papilar sobre válvula pulmonar en una mujer joven detectado por ecocardiografía y tratado mediante excisión quirúrgica con un postoperatorio sin complicaciones.
Papillary fibroelastomas (PFEs) are rare benign primary cardiac tumors that occur on the endocardium of the heart, usually depending on the heart valves. They account for approximately 7% of all primary cardiac tumors.1
Most of them have been described on the left side of the heart, but those depending of the right side are particularly uncommon, with only a handful of cases reported on the pulmonary valve.
Majority of patients with PFE remain asymptomatic and the tumors usually are an incidental finding resulting of the increasingly extended use of echocardiography.2
However, these tumors are a potential source of embolisms and obstructive phenomena and so they are responsible for life-threatening complications. Current literature stands for surgical excision as first choice treatment.1
We present a singular case of papillary fibroelastoma depending on the pulmonary valve in a young woman with no symptoms which was surgically removed.
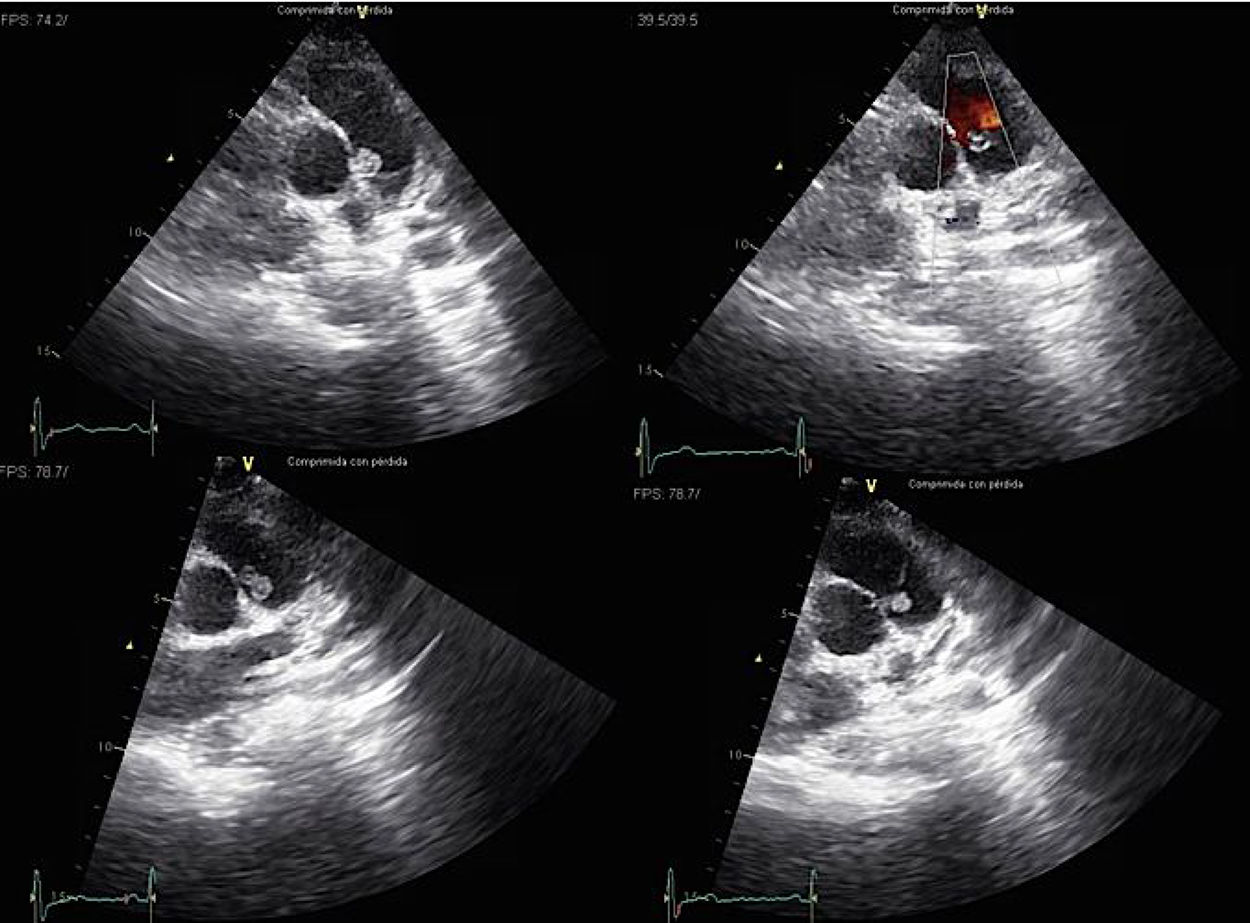
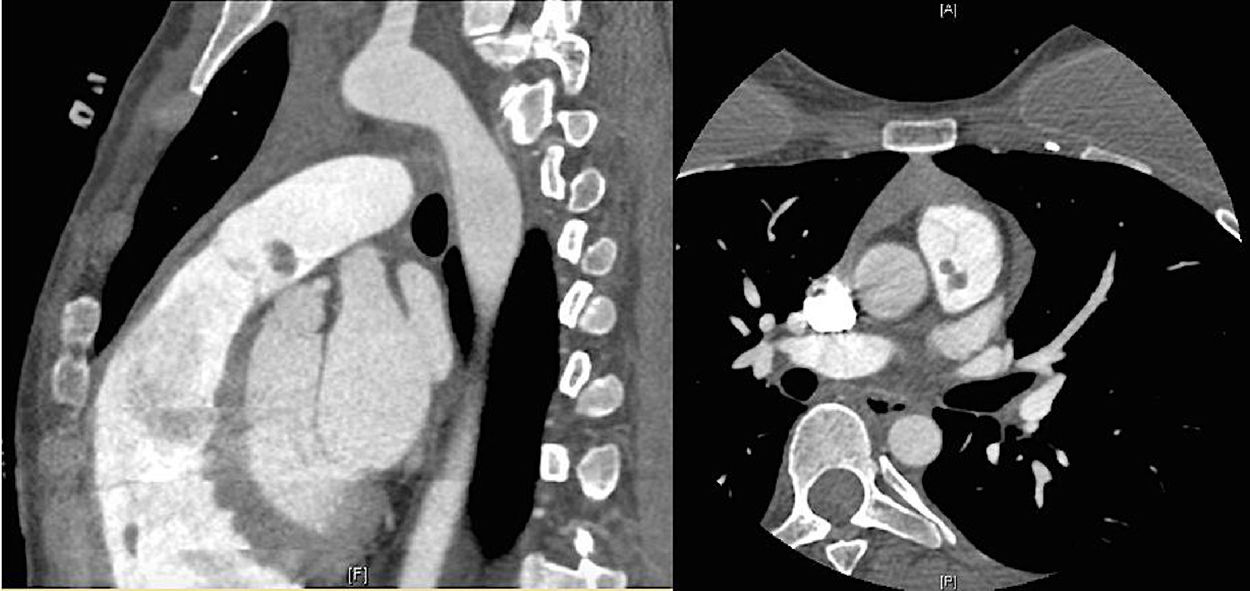
Case reportAn asymptomatic 30-year-old woman with no medical past history was medically referred to cardiologist because of a right branch bundle block finding in routinary electrocardiogram. She presented a systolic heart murmur and an echocardiography was performed. Transthoracic echocardiogram showed an intracardiac small mobile mass in main pulmonary artery (Fig. 1). Magnetic resonance imaging (MRI) and computed tomography angiogram (CTA) confirmed this finding (Fig. 2). Differential diagnosis contemplated an intracavitary thrombus or intracardiac tumor. The mass did not disappear after two weeks of systemic anticoagulation. A CTA as extension study was planned thinking of a likely neoplasm which did not show metastatic spread lesions.


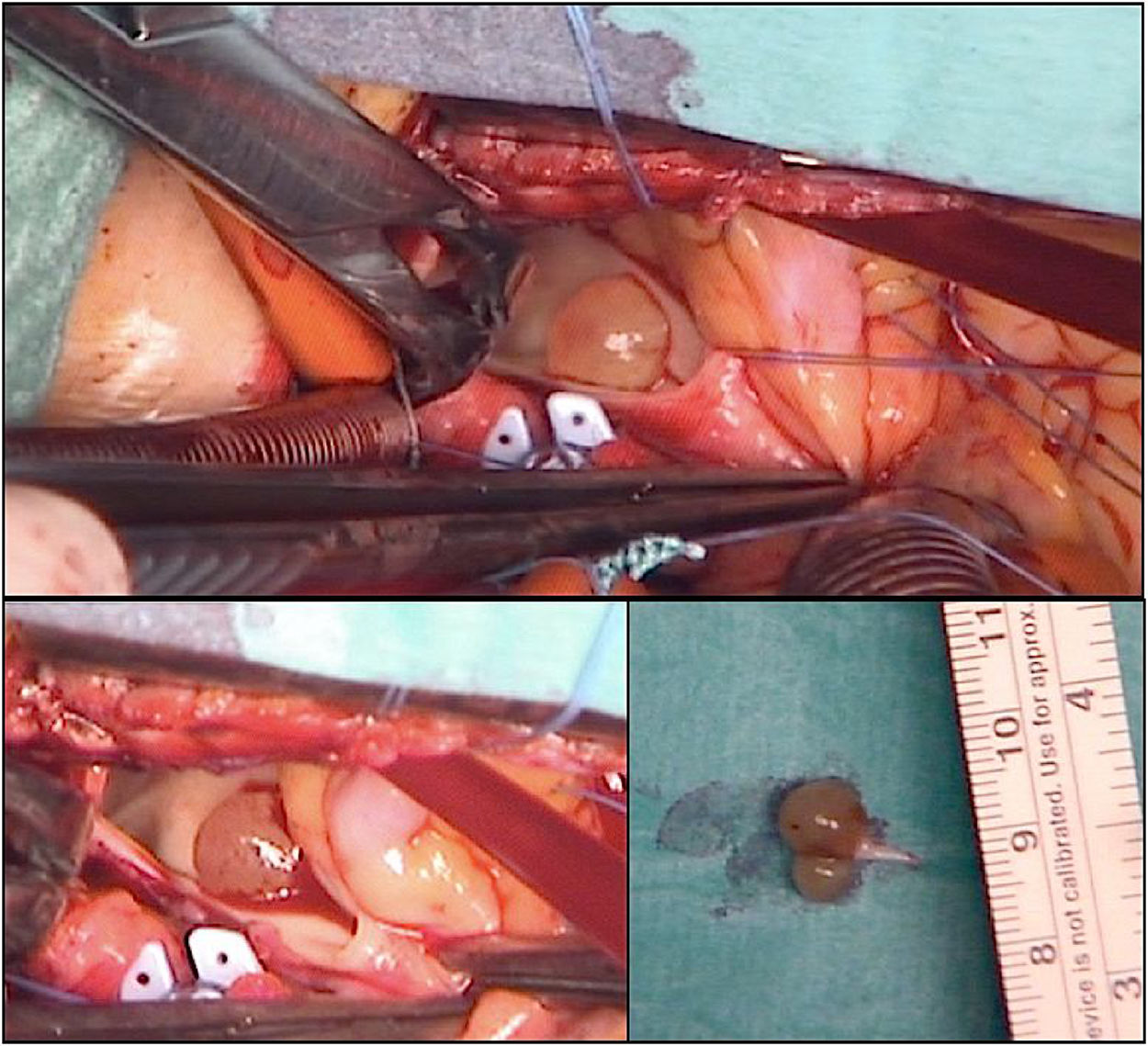
Priority surgery was decided for tumor excision and typing its nature. Through a median sternotomy cardiopulmonary bypass was established. A transverse excision was made on the pulmonary artery 2cm above the pulmonary valve. Through the incision a yellow, encapsulated and bilobulated 10mm×6mm sized tumor was identified (Fig. 3). It was attached by a pedicle to posterior leaflet of pulmonary valve, which was partially resected and reattached to the commissure.

Intraoperative histological study excluded malignancy. Pulmonary artery was closed without stenosis and cardiopulmonary bypass was weaned. Intraoperative transesophageal echocardiography showed mild pulmonary insufficiency with no hemodynamic repercussion and absence of residual tumors.
Postoperative course was uneventful and she was discharged at fourth postoperative day.
Definitive histological and pathological study revealed papillary fibroelastoma of the pulmonary valve with no margin affection.
DiscussionCardiac PFEs are uncommon cardiac benign tumors with an overall incidence said to be under 0.02%.3 They represent the most frequent primary valvular tumors in the heart, although they have been described depending on almost any cardiac structure including papillary muscles, chordae tendineae and endocardium. More than 95% arise in the left side of the heart. They have been most commonly observed in the aortic valve, followed by the mitral and the tricuspid valve. The pulmonary valve is rarely involved, with only 7% of PFEs described on it. The PFEs that originate from the semilunar valves may project into ventricular or arterial lumen and those originating on the atrioventricular valves project into the atria.1
Before the advent of echocardiography they were largely found incidentally during cardiac surgery or on necropsy studies.2
They clearly predominate in adults with mean age of detection at 60 years.4 These tumors are usually small with less than 20mm although tumors as large as 70mm have been described. They have a characteristic flower-like appearance attached to the endocardium by a short pedicle. Papillary fronds are narrow, elongated and branching. When placing the excised tumor in a saline solution typically results in a sea-anemone like appearance that provides a morphological verification of the tumor as a PFE.5,6
Histologically PFEs are covered by a single layer of endothelium, containing a core of connective tissue with mucopolysaccharide acid matrix, smooth muscle cells, collagen elastin fibers (which are the hallmark of this tumor), occasional cysts and areas of hemorrhage.6
The pathogenesis of theses tumors is still unknown although repetitive hemodynamic stress seems to play a role in it; yet no clear risk factors for PFEs development have been reported. It has been suggested an association with organizing thrombus, viral endocarditis, inflammatory changes, hamartomous origin or previous endothelial damage.3
Natural history of these tumors has not been well defined. Over 60% of PFEs are known to be asymptomatic and slow growing and usually represent an incidental finding. Nevertheless, they cause turbulent flow and thrombus formation with potential risk of systemic or pulmonary embolism or obstructive phenomena. They have been reported to cause coronary, cerebral, retinal and pulmonary artery embolisms and obstructions in literature.3,7,8 Tumor mobility has been the only independent predictor observed of PFE-related death or nonfatal embolization.1
A differential diagnosis between PFEs and leiomyosarcomas is helpful to plan the therapy strategies as the survival rates differ substantially. MRI is useful in preoperative surgical staging and helps to determinate the benign or malignant nature of the neoplasm.3,4
In a meta-analysis Gowda et al.1 documented a 50% cardiac PFE related mortality rate in patients who did not undergo curative resection for either systemic embolism or outflow tract obstruction. In order to prevent these complications, the gold standard therapy for PFEs is surgical excision, which is often curative, safe and presents good results.9
PFEs are rarely associated with valvular dysfunction, so they can be excised locally without the need of valve replacement. Excision of the valve should be as minimal as possible. Recurrence after surgical removal has not been yet reported in literature with the longest follow-up period reported of 11 years.1,10
ConclusionsIn conclusion, PFEs are rare cardiac benign tumors that are increasingly detected by echocardiography. Most of them are asymptomatic but they can cause life-threatening complications such as systemic or pulmonary embolism and obstructive phenomena. Surgical resection of the tumor is the most appropriate therapy and can be performed safely. A conservative valve-sparing approach is recommended because of the absence of recurrence after total excision with long-term excellent prognosis.
FundingNone.
Conflicts of interestThe authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.

