



Preparation process and life service solicitations can cause damage on concrete's internal structure, creating cracks that tend to propagate and increase with time. This poses a risk of failure as water penetrates, corroding the rebar reducing concrete's life span. Cement can exhibit up to a certain extent a natural ability to self-heal, consequence of the long-term hydration phenomenon. Some initial cracks can be spontaneously closed if the right conditions are met (humidity). However, it will not be enough to repair major cracks formed internally over a long period of use, so strategies need to be developed to achieve an efficient level of self-healing. This need lead to a new concept – self-healing. The biological approach is a suitable alternative to achieve healing in concrete. In this work, bacteria were immobilised in expanded clay and added to concrete by aggregate replacement.
Sustainability has been a key driving force within construction in recent years. Non-renewable natural resources i.e. coal, oil, metal ores, have been depleting at an alarming rate, due to supply and demand in all industries throughout the world [1,2]. The onus on construction industry to deliver projects that meets high quality standards and sustainability criteria are extremely high. The construction sector has taken steps to minimise the use of non-renewable materials and one of these materials is concrete [3,4]. This unique material has been used for more than one century and the development of concrete has come a long way since. Many variations have been trialled throughout the years to understand, and expand upon, its use. Today, it is usually made up of four main constituents – binder, aggregate, water and admixtures. To increase the strength of concrete, generally more cement needs to be included. Large strides have been made in turning concrete into a more sustainable material [5]. Concrete has many qualities, ranging from its high strength and ability to withstand natural disasters, to its versatility and low maintenance. It is because of these many qualities that concrete remains an essential component when it comes to construction design, however its high susceptibility to crack remains unsolved, [6]. Structural failure of concrete has been one major concern in industry. The standard approach has been to prepare stronger concrete, a non-sustainable solution with high environmental impact. Search for a more sustainable and durable concrete, less prone to cracking, lead to a new concept – self-healing [7,8]. This concept, inspired by the natural ability of plants and human skin to spontaneously heal, inspired researchers to search for a method of conferring concrete with the ability to self-repair internal damage [9].
Preparation process and life service solicitations can cause damage on concrete's internal structure, creating cracks that tend to propagate and increase with time. This poses a potential risk of failure as water infiltrates and allows for chloride ion penetration, corrosion of the rebar, amongst other problems – considerably reducing concrete's life span. It is known that cement can exhibit, up to a certain extent, a natural ability to self-heal, a consequence of the long-term hydration phenomenon. Hence, some initial cracks can be spontaneously closed if the right conditions are met – concrete's incomplete saturation, presence of residual clinker and crystallisation of calcium carbonate [10].
This, however, will not be enough to repair most of the major cracks that are formed internally over a long period of use, so strategies need to be developed to achieve an efficient level of self-healing.
The development within this field has led to the investigation of different routes. Looking at the several studies conducted so far, the main methods to achieve self-healing can be pointed out as being:
- •
Precipitation of calcium carbonate CaCO3[11,12]
- •
Promoting continuing hydration using admixtures [13,14]
- •
Use of encapsulated healing agents [15]
- •
Use of shape memory materials (SMM) [16]
Chemical and biological self-healing involves the addition of an extra element, not included in the original mix design. This additive triggers a reaction mechanism and products from the process are responsible for the crack closure. The biological approach has been presented as a suitable alternative to achieve healing in concrete and it is the one presented and discussed in this research work [17].
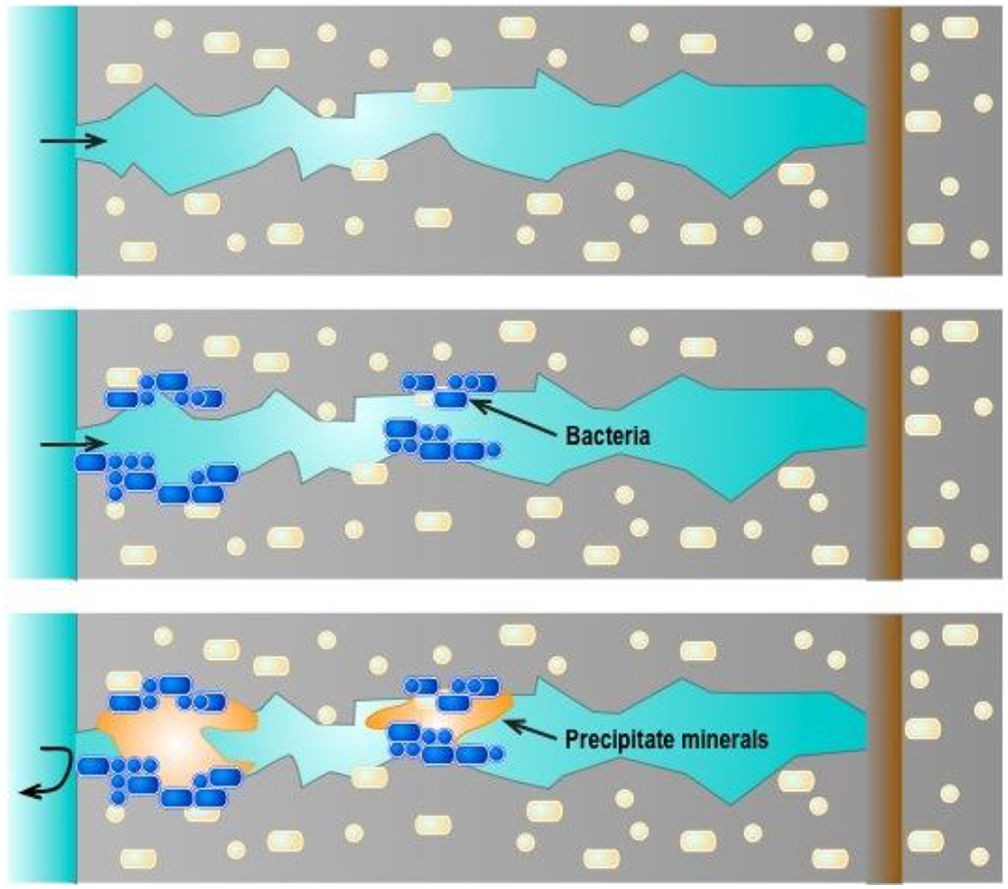
Jonkers describes the mechanism of adding bacteria to concrete, a process that through the addition of ingress water, allows the conversion of calcium lactate to calcium carbonate (limestone) which results in the crack sealing (Fig. 1) [18]. Due to the high PH level conditions found within concrete, the bacteria infused within the structure can remain dormant for, depending on the type of strain, 200 years [19]. It is only when cracks start to form and water seeps in, that PH lowers and the bacteria are activated [20].

The reaction mechanism can be described by the following equation [21]:
The CaCO3 (limestone) compound can, not only be formed through the natural process, but also through this microbial metabolic operation. This formation can be directly related to a human biological feature, the repairing of bone post-fracturing. However, selecting the bacteria that will be most effective is a demanding task.
When conducting research into finding the correct bacteria, scientists initially had to find a species that had the capability of being able to endure high alkaline conditions. When water and cement combine, they create a PH level that can reach as high as 13. For many bacteria, and organisms alike, this type of environment is too harsh to survive. Results showed that a certain strain of bacteria, namely Bacillus, seemed to flourish in notably severe conditions [19,20]. In addition, it is not only the sourcing of viable bacteria that scientists have been trying to uncover but also acquiring a convenient food source. The food source that is required, not only has to be relevant to the specific bacteria at hand, but also has to last a long time within the concrete before the bacteria become active [22].
Numerous experiments on its use have found a significant increase in compressive strength, post-cracking, in comparison to controls groups [23]. Furthermore, it is noted that the limestone created via this process, may increase the concrete resistance to free–thaw cycles, preventing any future cracks that may arise. Another potential advantage is that the permeability of the structure will also decrease and corrosion of reinforced concrete will be lower, as the limestone will seal routes for further water ingress to occur [24,25]. The process does have some constraints though. This addition of large quantities of bacteria will bring a cost; in some case almost double that of conventional concrete [22,26].
The two main approaches to harbouring the immobilised bacteria within the concrete are the use of expanded clay and encapsulation in polymers. Jonkers et al. showed that the protection that expanded clay particles could give to the bacteria, would greatly expand their shelf life [27,28]. The clay would encapsulate the bacteria and conceal it for an extended length of time. In order to introduce the expanded clay, some, or all, of the aggregate would be replaced within the concrete, depending on the type of concrete required. This change in aggregate would lower the overall compressive strength of the concrete, due to the more hardened and dense gravel being lost. Nevertheless, even with the initial loss in compressive strength, it was found that the autonomous healing of the substrate greatly outweighed that of the gravel compound. The process seems feasible and the dispersion of the clay throughout the entire concrete mix proved to be possible. However, the even distribution of the clay particles still needs to be addressed, along with the ability of clay to withstand heavy forces during the mixing and pouring of industrial-sized quantities.
The capsule method follows the same principle as with the aforementioned encapsulation in expanded clay. The healing agent is contained by the capsule membrane and will only be released when a crack has penetrated the capsule wall [29]. Unlike the clay, the capsules are an additive rather than a replacement for any of the major constituents. This therefore allows the initial compressive strength of the concrete, pre-crack, to remain high as the gravel aggregate will still be included. The encapsulation of bacteria within the capsule is not an easy process, in comparison to the expanded clay. Specialised laboratory equipment is required, which in turn brings its own additional costs.
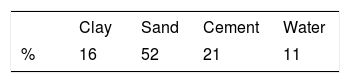
2Experimental2.1Materials and formulationsThe concrete cubes were prepared with a mix of ordinary Portland cement CEM I 42.5N, pit sand with a particle size up to 10mm, expanded clay and water according to Table 1. This would give a water cement ratio of 0.52. The expanded clay used was Liapor with a particle size between 1 and 4mm, supplied by Weber.
To ensure a thorough mix had been achieved for all trial groups, before casting took place the following mixing method was adopted:
- •
The cement and sand were manually combined thoroughly,
- •
Next the expanded clay was added and manually mixed,
- •
The water was added in stages, to ensure all components were bound well within the mix, during mechanical mixing for 2min.
To keep consistency, when casting all mixes, they were subsequently placed on the vibrating table for 30s to even out the distribution within the mould.
The alkali-resistant bacteria selected derives from alkaliphilic bacteria of the genus Bacillus and organic mineral compounds. The preparation of the expanded clay with bacteria has followed the method previously described by Tziviloglou et al. [30]. Calcium lactate, yeast extract and bacteria spores were impregnated under vacuum in particles of expanded clay. The clay was then dried until reach a constant weight.
2.2TestsCompression testing was carried out using an Avery Denison testing machine type 7226CB calibrated in accordance with BS 1610: Part1:1992. Load was applied at the rate of 2.5kN/s through the steel plates on which the specimen was placed.
XRD analysis was performed using a D8 Advance X-ray diffractometer (Bruker, Coventry, UK) equipped with Lynx Eye detector. The microstructural characterisation was conducted with a scanning electron microscope Hitachi SU8030 FEG-SEM, Japan, Thermo-Noran (USA) with an EDX system with 30 mm2 Ultra-Dry window and Noran 7 software. Noran 7 includes COMPASS principal component extraction and XPhase analysis techniques for evaluation of elemental distribution.
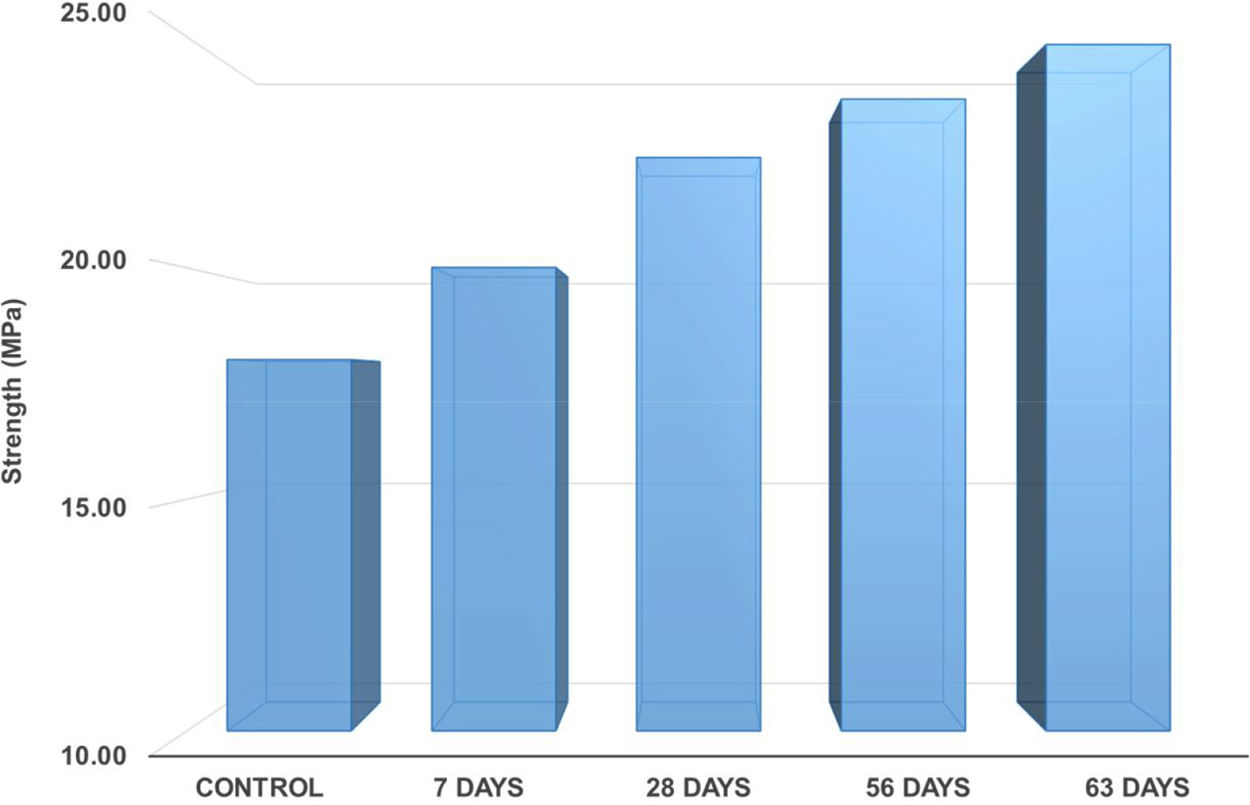
3Results and discussion3.1Self-healing testsBefore starting with the self-healing tests, it was necessary to determine the compression strength of a group of control samples to establish the force required to cause microcracks into the concrete samples. A trial group of samples was tested until failure reaching an average compression force of 23.7MPa. For the concrete samples with incorporated bacteria, the microcracks, detected through the microcontroller system of the equipment, appeared when 90% of the force was used, 21.2MPa. This was the force applied to pre-damage the samples before healing. These samples where then tested to failure after 7, 28, 56 and 63 days of healing. A group of control samples containing expanded clay without bacteria was also damaged and tested after the same healing intervals.
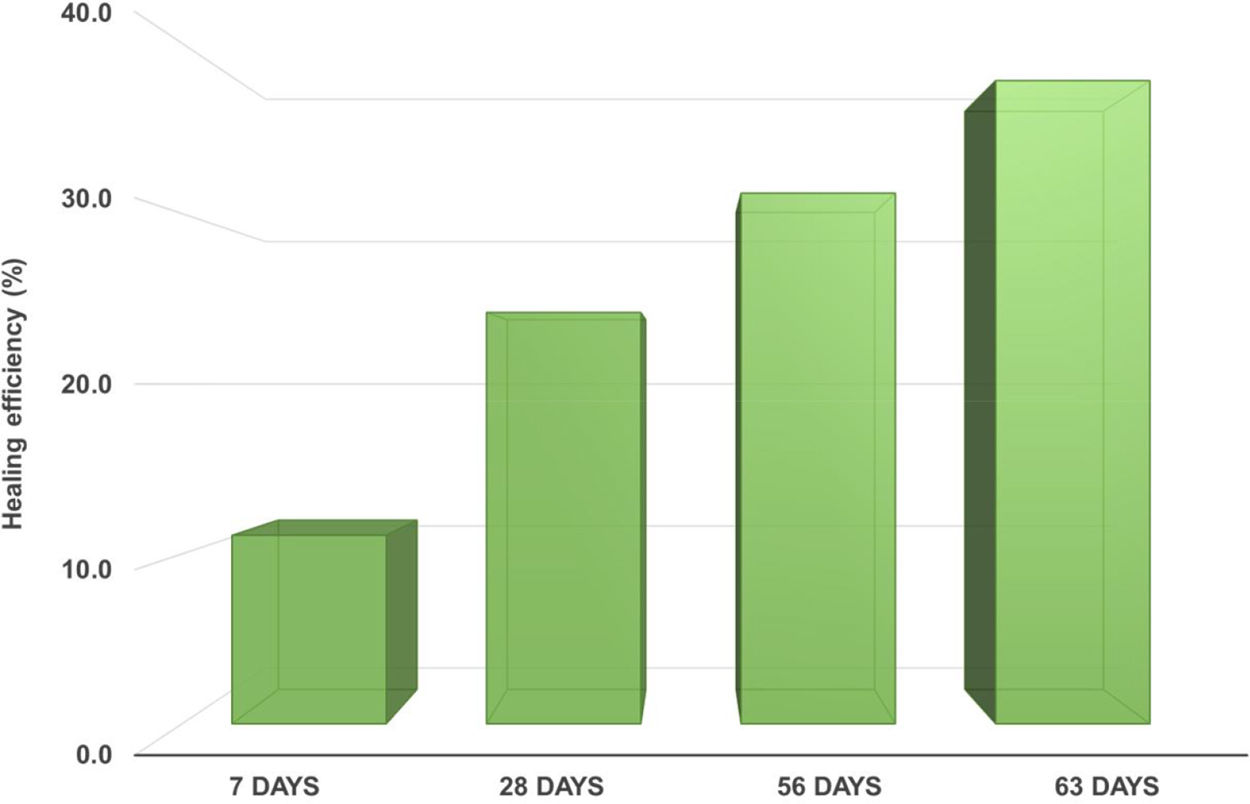
The assessment and quantification of healing has been one of the most challenging and important aspects in these materials. Different authors have explored diverse methods and no standard process has been made available so far [7]. Self-healing in this work was determined following the equation:
where Fc is the compression strength for the control sample and Fh is the compression strength for the healed sample.
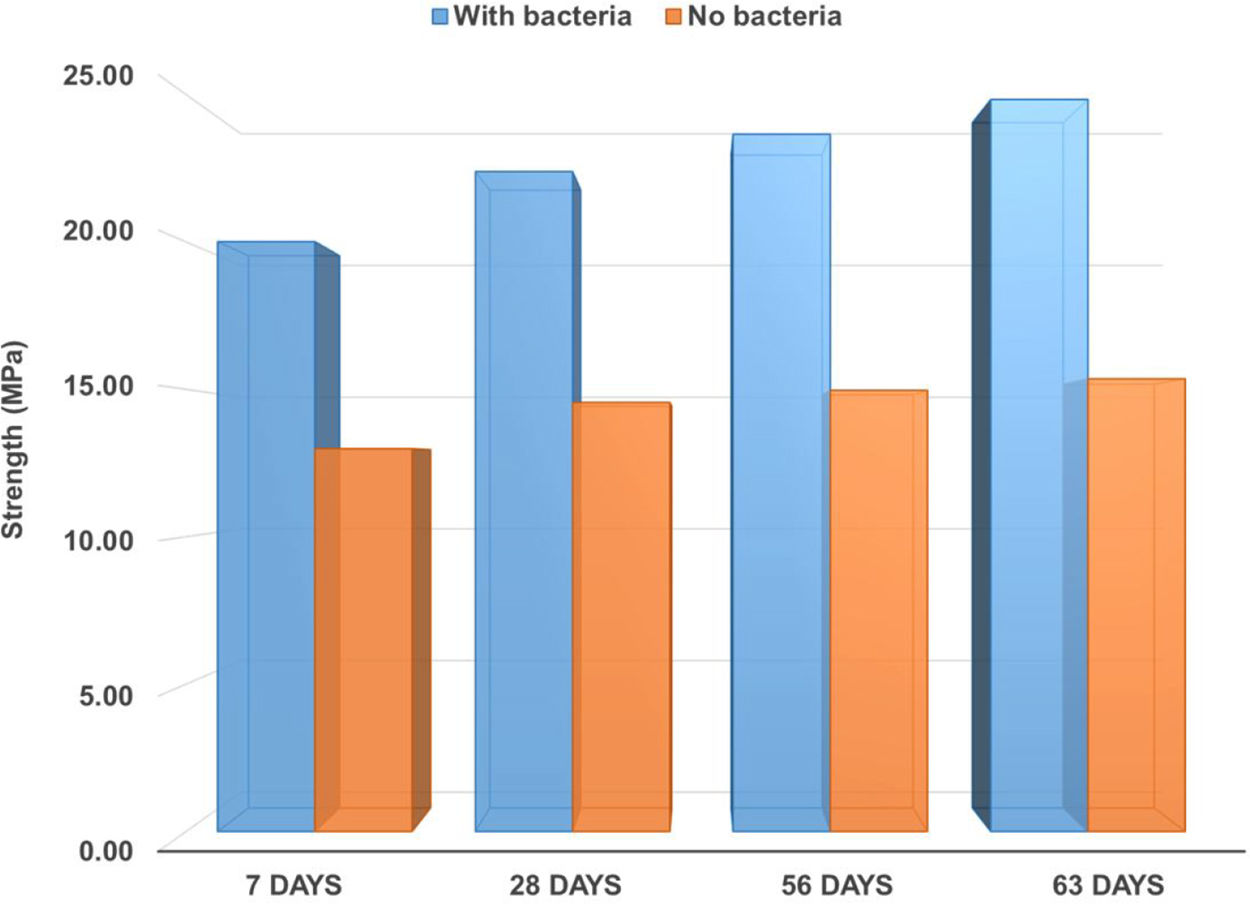
Concrete containing bacteria encapsulated in expanded clay shows an increase in the compressive strength after only 7 days of healing (Figs. 2 and 3), which translates into a healing efficiency of around 10%, at this stage (Fig. 4). When the results are compared with the control samples it is clear that the strength increase is caused by the presence of bacteria in the expanded clay. The samples containing solely expanded clay, without bacteria, show some improvement in mechanical strength from 7 to 28 days – which is expected from the normal hydration process of concrete – followed by practically constant strength after this period, when it reaches a plateau.



This is a quite remarkable effect considering that early strength development is particularly important in concrete. However, the highest recovery in strength is, as expected, achieved at a later stage, 63 days. These results confirm that the presence of bacteria can indeed contribute to the recovery of strength in concrete after it has been damaged. According to Fig. 4, healing efficiency after 63 days reaches almost 40% what indicates that the self-healing samples exhibit long-term hydration, promoted by the presence of bacterial activity.
To confirm if this recovery was caused by the action of the bacteria, producing limestone, the samples were analysed by scanning electron microscopy, EDS and XRD analysis. Fig. 5 shows the presence of the characteristic ettringite crystals and calcium carbonate, CaCO3.

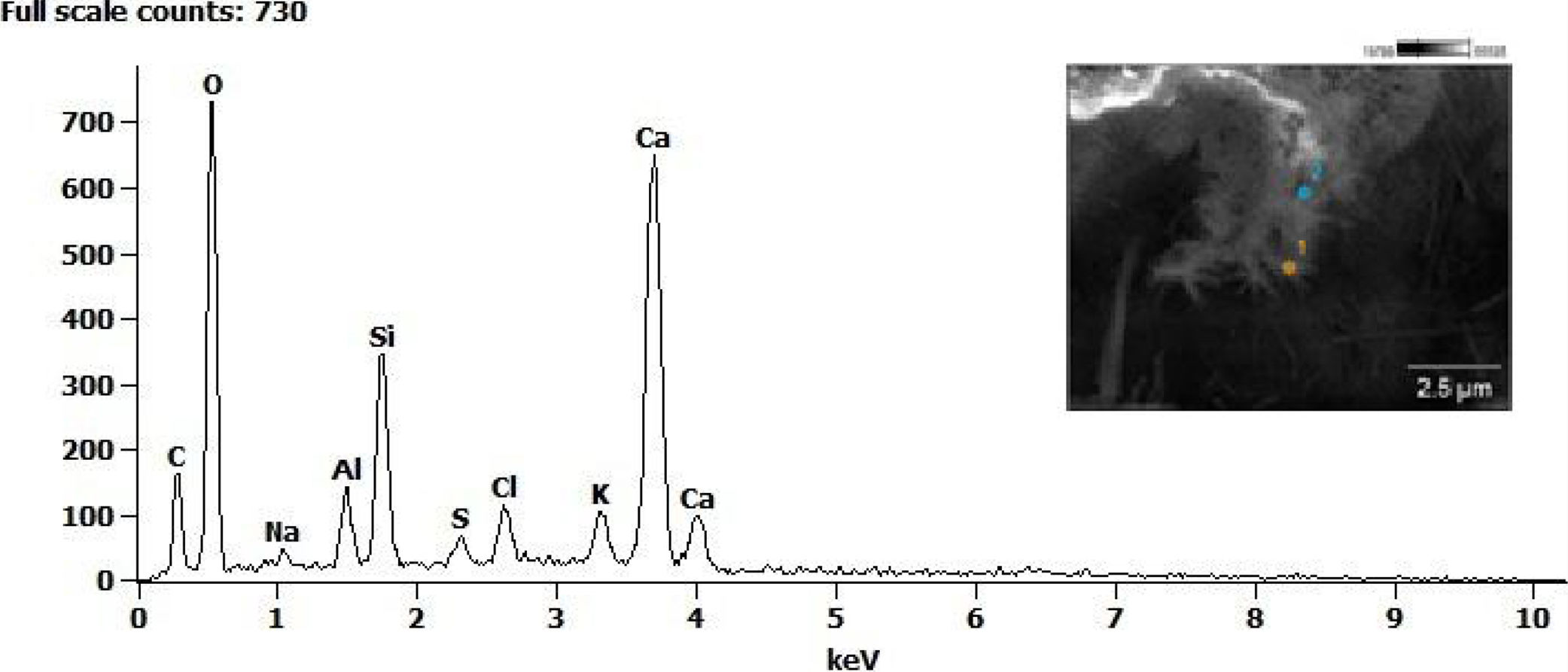
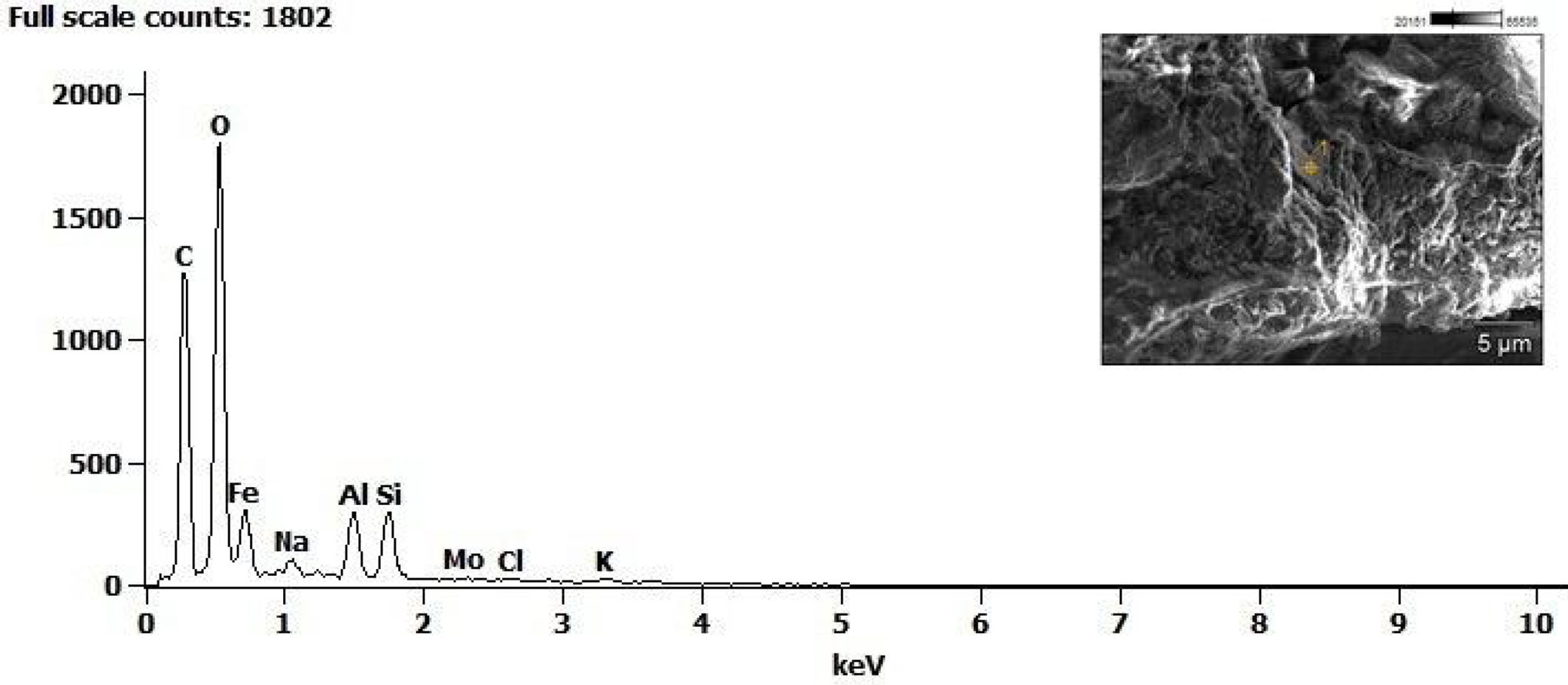
The study of the precipitates formed in a crack surface conducted using EDS analysis revealed a strong presence of calcium, oxygen and carbon (Fig. 6) while the cracks in a control sample do not show any calcium (Fig. 7).


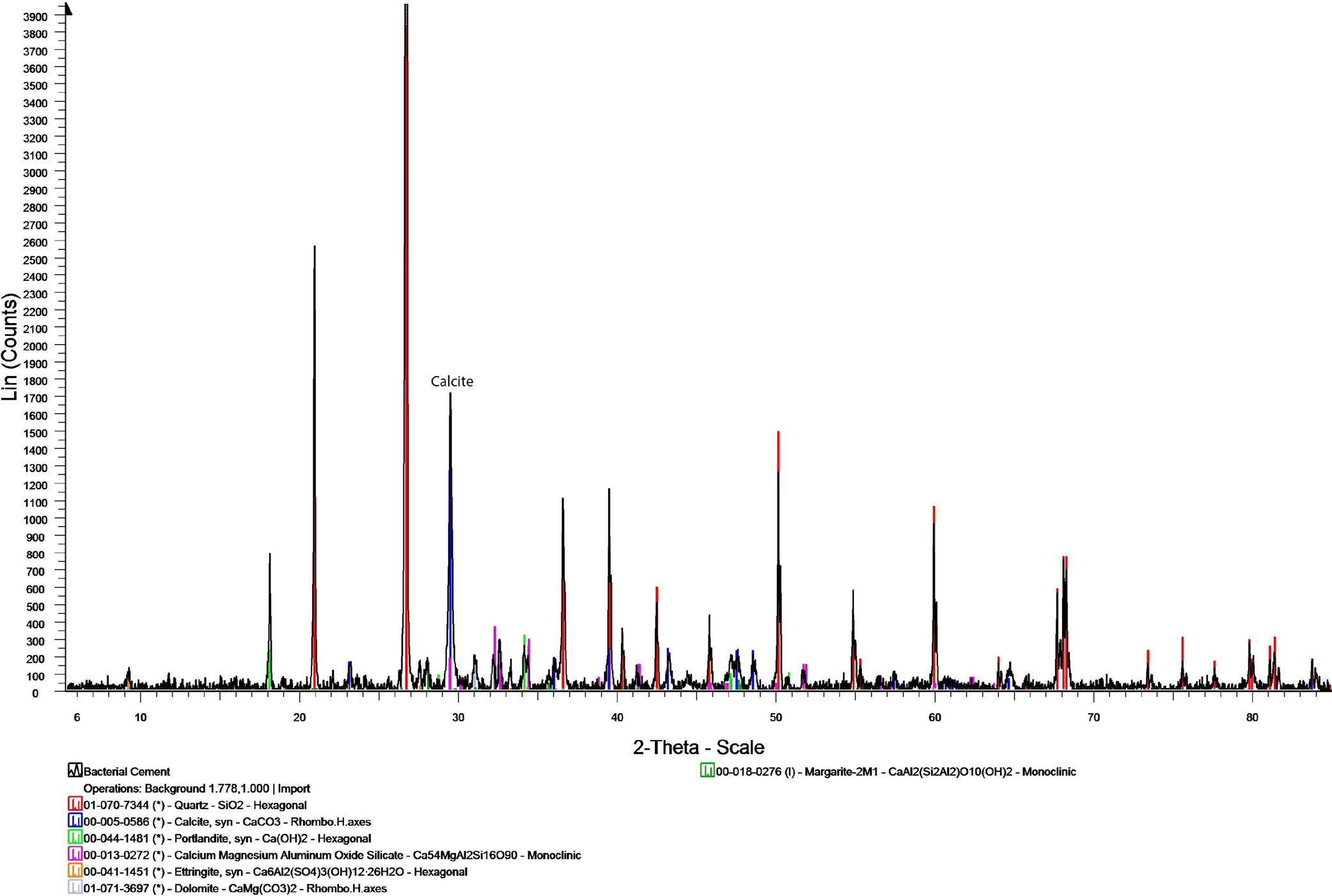
Samples from the concrete containing bacteria were also tested using X-ray diffraction. The results, in Fig. 8, confirm the presence of calcite (peak C), the product of the reaction mechanism triggered by bacteria activity within the samples.
4Conclusions
The results obtained with the tests conducted in this study confirmed that the replacement of aggregates with expanded clay impregnated with bacteria could effectively contribute to strength recovery in concrete. It has been demonstrated that the recovery has been in fact caused by the presence of calcium carbonate, the main reaction product resulting from the bacteria activity.
Although further studies are required to estimate the longevity of the bacteria and the durability of this concrete, the results demonstrate its feasibility.
The authors would like to acknowledge the Delft University of Technology for the support providing the bacteria for the tests and Weber Saint-Gobain UK for supplying the expanded clay.
