





Odontomas are odontogenic benign tumors composed of dental tissue. Most of these lesions are asymptomatic and are often detected on routine radiographs. Morphologically odontomas can be classified as complex, when present as irregular masses containing different types of dental tissues, or as compound if there is superficial anatomic similarity to even rudimentary teeth – the denticles.
A 9-year-old girl attended our Dental Medicine appointment with doubt about the apparent delay in exfoliation of deciduous teeth: 53–55. A panoramic radiograph showed the presence of a lesion formed by many radiopaque small tooth-like structures constituting an obstacle to the respective permanent teeth eruption. Under general anesthesia, access to the lesion was achieved via intra-oral approach and its surgical removal was performed. The histopathologic examination confirmed the diagnosis of compound odontoma.
Routine radiographic examination is important for early detection of silent lesions such as odontomas.
Os odontomas são tumores odontogénicos benignos compostos por tecidos dentários. Normalmente são lesões assintomáticas, constituindo achados radiográficos. Quanto à sua morfologia os odontomas podem ser classificados como complexos, quando se apresentam como estruturas com distribuição irregular dos diversos tipos de tecidos dentários, ou como compostos quando esses tecidos se encontram organizados originando estruturas rudimentares semelhantes a dentes - os dentículos.
Uma menina de 9 anos de idade veio à nossa consulta de Medicina Dentária apresentando preocupação quanto ao aparente atraso na erupção dos dentes 53, 54 e 55. Após realização de uma ortopantomografia, foi detetada uma lesão formada por várias estruturas radiopacas semelhantes a dentes, que constituía um obstáculo à erupção dos respetivos dentes permanentes. A lesão foi removida por via intra-oral sob o efeito de anestesia general.
O exame anatomopatológico confirmou o diagnóstico de odontoma composto.
Os exames radiográficos de rotina são fundamentais para a deteção precoce de lesões silenciosas como os odontomas.
The term odontoma (or odontome) was originally used by Paul Broca in 1867 to describe all odontogenic tumors.1 Presently this term is circumscribed to benign lesions of odontogenic origin and a mixed character composed of dental epithelial and mesenchymal cells. Due to their composition and behavior, odontomas can be regarded as hamartomas or malformations rather than true neoplasms.1–3 These malformations do not develop further once fully calcified but, like teeth, they may erupt into the mouth.4 This is, however, a rare situation. They are characterized by their slow growth and non-aggressive behavior.5,6
Histologically, odontomas are composed of different dental tissues, including enamel, dentin, cement and, in some cases, pulp tissue.7 These dental tissues may appear normal but they seem to have a deficient structural arrangement.
Odontomas are mainly intraosseous lesions although location in gingival soft tissue has been reported. There are very few reports of odontomas associated with primary teeth in the literature. In general, odontomas occur more often in the permanent dentition. The lesions tend to be located between the roots of erupted teeth or between the deciduos and permanent teeth. Anterior maxilla, followed by anterior mandible and postero-inferior regions are the most common locations.8
Epidemiologically, odontomas are the most frequent odontogenic tumors, and according to different sources in the literature, it accounts for 22–67% of all maxillary tumors.7,9 Males and females are approximately equally affected.3,7–10 An increased prevalence of these tumors can be found in children and adolescents.9
The etiology of odontomas is unknown, but it could be due to trauma during primary dentition, as well as to inflammatory and infectious processes, hereditary anomalies (Gardner's syndrome,3 Hermann's syndrome), odontoblastic hyperactivity, or alteration of the genetic components responsible for controlling dental development.9,11
According to the 2005 classification of the World Health Organization (WHO),11 two types of odontomas are acknowledged: (a) compound odontomas that usually are unilocular lesions containing multiple radiopaque, miniature tooth-like structures known as denticles; and (b) complex odontomas that consist of an irregular mass of hard and soft dental tissues. Compound odontomas are approximately twice as common as complex Odontomas.1,5,7,11
Odontomas are usually asymptomatic, and they may be detected by chance on a routine radiograph (panoramic and/or intra-oral X-rays), or when they are large enough to cause a swelling of the jaw. Clinical signs suggestive of an odontoma include a retained deciduous tooth or an impacted tooth.8,10
Surgical removal is the treatment of choice.10 Care should be taken, however, not to harm adjacent teeth and permanent germens in children, while follow-up is essential for evaluation of further development of the permanent dentition at the removal location. Although the diagnosis of odontomas, in most cases, can be provisionally confirmed by radiographic examination, a histological study of the removed lesion must be done to confirm the diagnosis.12
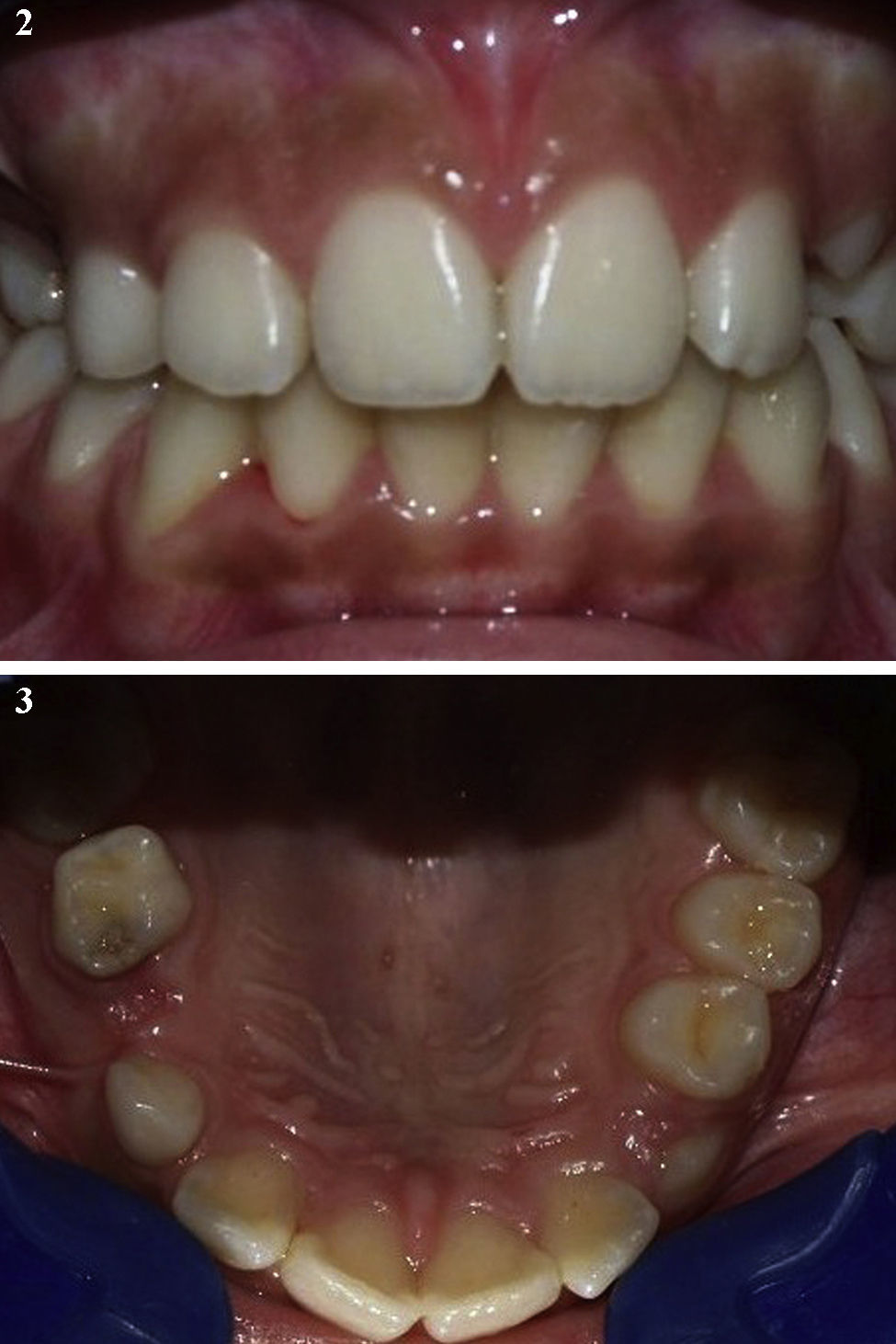
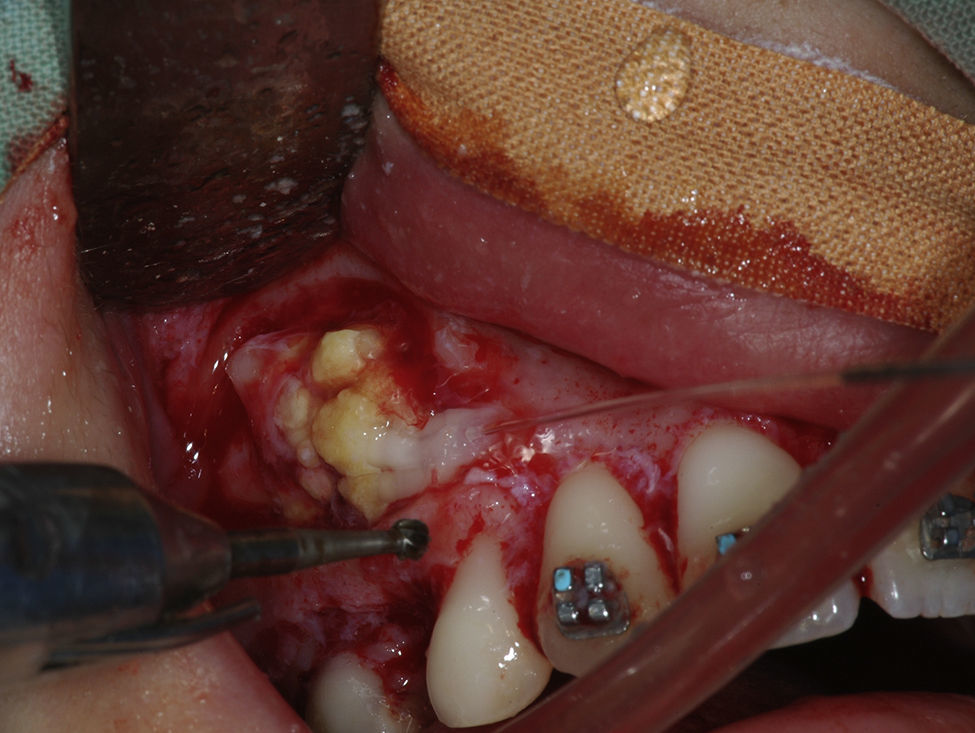
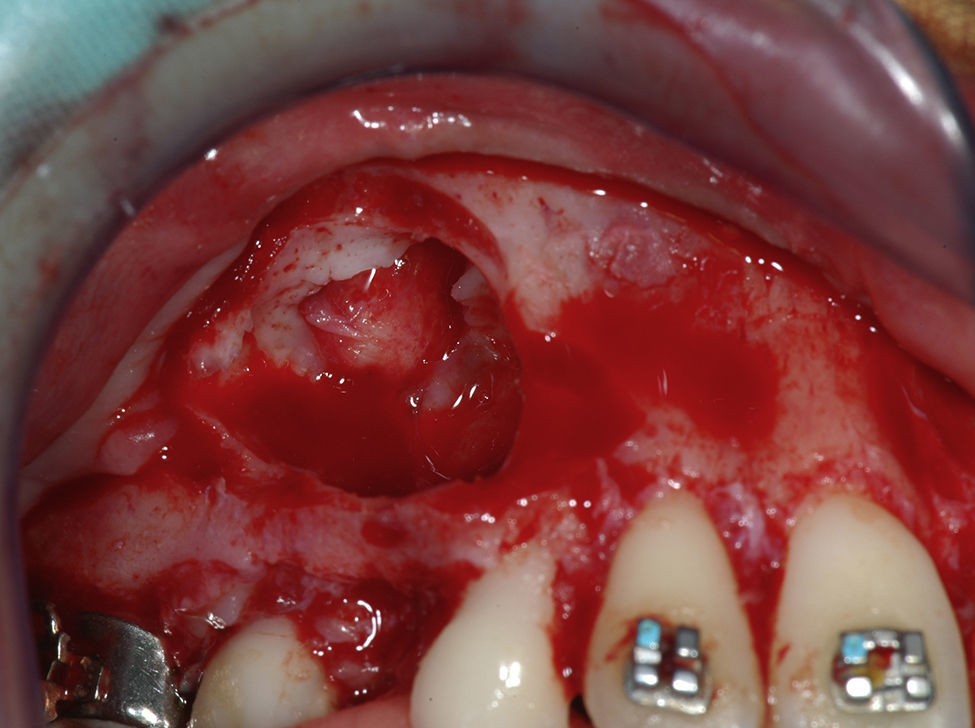
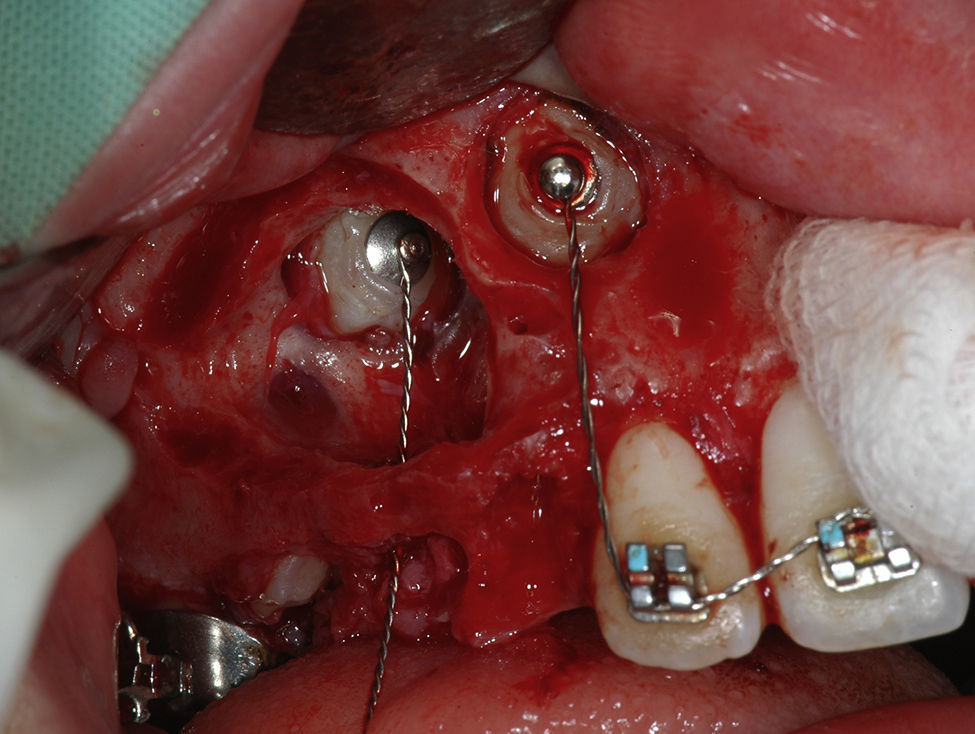
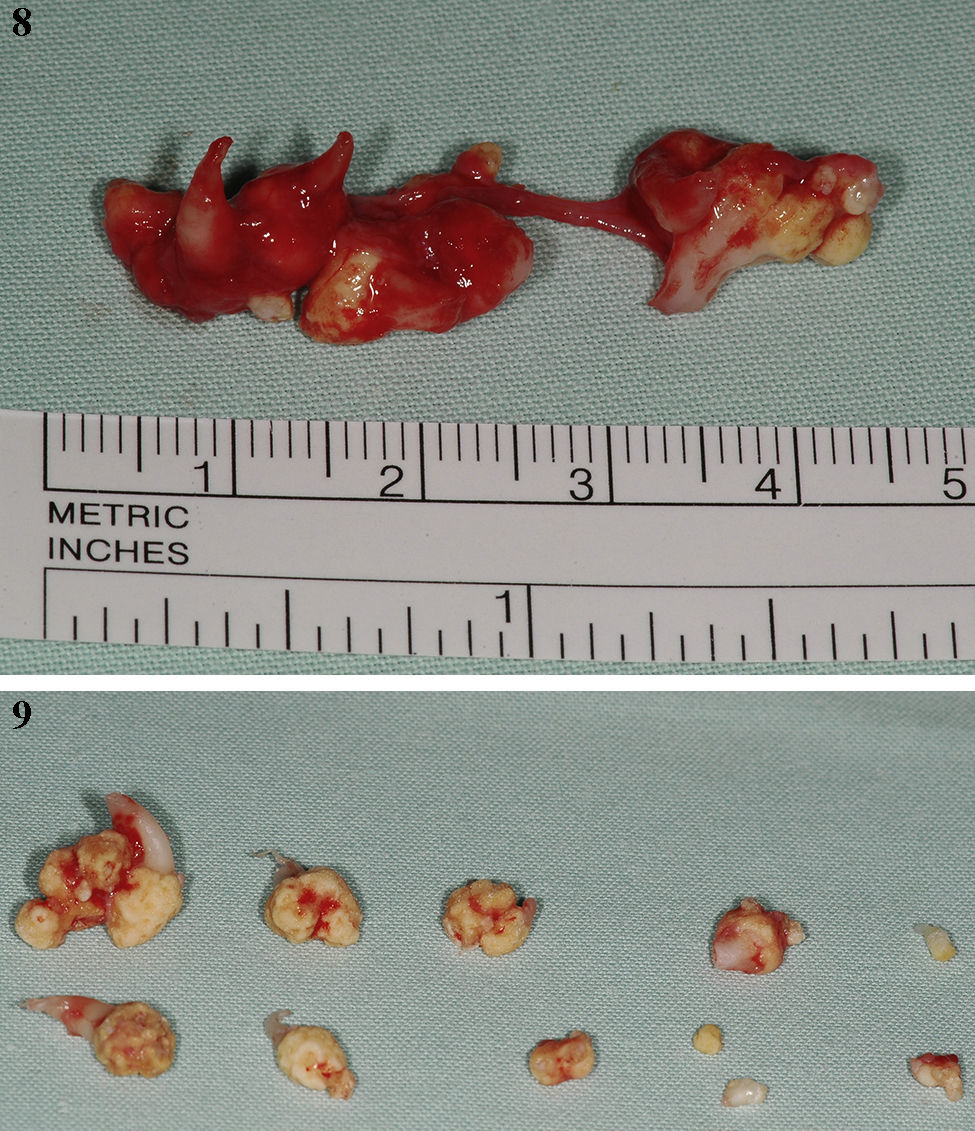
Case reportA 9-year-old female patient attended our Dental Medicine appointment with doubts about the apparent delay on the exfoliation of the upper right deciduous teeth. The clinical history did not reveal any systemic pathology associated. Intraoral examination revealed the presence of the primary teeth 53–55 and the absence of the corresponding teeth in the other quadrants, with the exception of tooth 63, already with mobility. A panoramic radiograph (Fig. 1) was obtained, which revealed the presence of multiple small radio opaque tooth-like structures in the apical region of 53 and 54, surrounded by a narrow radiolucent area. These structures have disrupted eruption of the respective permanent teeth. The patient was asked to take a computerized axial tomography, in order to assess the location and relationships of the lesion. During this period the teeth 54 and 63 had exfoliated (Figs. 2 and 3). These tooth-like structures were carefully excised, as well as teeth 53 and 54, under general anesthesia, without disturbing the unerupted teeth (Figs. 4–6). The impacted teeth 13 and 14 had an orthodontic device for traction attached during the operation (Fig. 7). Specimens were then sent for histopathological examination which confirmed the diagnosis of compound odontoma (Figs. 8 and 9). The young patient was regularly examined, and one month after surgery a panoramic radiograph (Fig. 10) was taken to control eruption of 13 and 14, which were already in a more occlusal position.








Several case series have documented that the majority of all odontomas were diagnosed in the first two decades of life.8 Although they may be discovered at any age, less than 10% are found in patients over 40 years old. Some studies have reported a correlation between patient age and the type of odontoma involved – compound lesions being apparently more frequent in younger patients,10 which is in agreement with our case.
Discovery often occurs due to radiographic investigation for the cause of a non-erupted permanent or retained primary tooth.8,10 An impacted tooth is present in more than half of the cases.10 In the 26 cases of odontomas analyzed by Iatrous et al.,12 80.7% had the impaction of permanent teeth associated. In our case the lesion was found due to a delay on the exfoliation of teeth 53 and 54. When a panoramic radiograph was taken an irregular radiopaque image with variations in contour and size, composed of multiple radiopacities corresponding to the so-called denticles, could be seen.
Most authors agree that these lesions effectively appear more often in the upper maxilla, though some sources make no distinction between the two maxillas.1,9 In our case the odontoma was located in the upper jaw, what is in accordance with the first theory. The reported tendency of odontomas to arise in the region of the incisors and canines9 is also confirmed in our case. Interestingly, both types of odontoma occurred more frequently on the right side of the jaw than on the left.13
Considerable controversy exists over gender distribution. While some studies consider odontomas to be more common in females than in males,14,15 others consider these lesions to be similarly distributed between both genders.7–10 On the contrary, Iatrous et al.12 and Yadav et al.2 found a male prediction.
Ameloblastic odontoma and ameloblastic fibroodontoma bear great resemblance to the common odontoma, particularly on a radiograph, and thus it is suggested that all Odontomas should be sent to an oral pathologist for microscopic examination and definitive diagnosis.1,2,12,13
Odontomas have been associated with trauma during primary dentition, as well as with inflammatory and infectious processes, hereditary anomalies (Gardner syndrome, Hermann's syndrome), odontoblastic hyperactivity and alteration in the genetic components responsible for controlling dental development.9,12 In our case no syndromes were evident and no episode of previous trauma was reported by the patient and family.
In children, the impacted permanent teeth, depending on the age and on the tooth development, may be left to erupt spontaneously, or they may be guided to occlusion via orthodontic traction. In any case, follow-up is essential following odontoma excision.16,17 In our case due to the apical location and position of teeth 13 and 14, orthodontic therapy was applied at the same time of the surgical removal of the lesion.
ConclusionWe present a case of a compound odontoma associated with impaction of two permanent teeth – canine and first bicuspid. There is a high association between odontomas and permanent teeth impaction. In order to prevent the adverse effects of disturbances in tooth eruption the authors stress upon the importance of routine use of panoramic radiography for early detection of such dental abnormalities.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence must be in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors gratefully acknowledge the collaboration of Prof. Ana Portela (FMDUP) in the pre-surgical orthodontic preparation of the case and in the collage of orthodontic buttons during the surgery.