




fiteBac Skin Softening Gel, widely used as a cosmetic, contains the anti-infective benzalkonium chloride embedded in siloxane quaternary ammonium compounds, but does not contain alcohol. It thus serves well for skin protection combined with local anti-infective activity. As it does not penetrate the skin, no systemic toxic side effects are expected, and more than 3 years of practical use have not revealed any adverse reactions.
We have tested in a pilot study the usefulness of fiteBac Skin Softening Gel against skin lesions following insect bites various in nature as well as a few other ailments (e.g. fungus-related intertrigo). Of the 23 cases tested, all but one responded to the treatment with complete resolution of skin lesions within a few days up to a week. The only exception was a case of suspected tick bite with local arthritic symptoms. In the latter, a combination of the fiteBac gel treatment with subsequent local administration of ibuprofen gel also resulted in complete remission of dermatitis and arthritis.
We thus recommend wider use of this cosmetic/anti-infective agent for the prevention and treatment of insect bites to prevent subsequent infectious complications (such as, for instance, Lyme disease).
El gel fiteBac suave para piel, ha sido ampliamente empleado como cosmético, contiene cloruro de benzalconio y está integrado con compuestos de amoniaco cuaternario en silicona como anti-infeccioso, pero no contiene alcohol. Por lo tanto, sirve para la protección de la piel combinado con una actividad local anti-infecciosa. Como ésta no penetra la piel, no se esperan efectos secundarios, y en más de tres años de su aplicación no se han revelado reacciones adversas.
Se ha probado en un estudio piloto la utilidad del gel suavizante de piel en lesiones causadas por piquetes de insectos de diversa naturaleza, así como en otros padecimientos. (ej. micosis-relacionada con intertrigo). De 23 casos, todos menos uno respondió al tratamiento con la resolución total de las lesiones en la piel en unos cuantos días a una semana. La única excepción fue un caso con sospecha de mordedura de garrapata y síntomas de artritis local. Este último, la combinación del tratamiento con gel fiteBac y aplicación posterior de gel de ibuprofeno ayudó a la completa remisión de dermatitis y artritis.
Por lo anterior, se recomienda un uso más amplio de este agente cosmético/anti-infeccioso para la prevención y tratamiento de picaduras de insectos para evitar complicaciones infecciosas subsecuentes. (Como, por ejemplo, la enfermedad de Lyme).
Insect bites and stings may lead to transmission of pathogenic organisms and, in severe cases, are even treated as a medical emergency.1–4 Many of these are accompanied by secondary exanthema of various kind.5 Treatment commonly is done by epinephrine, diphenhydramine and steroids. Oral antibiotics may be given for infected bite wounds.6,7 Next step is to obtain a definitive diagnosis and to initiate appropriate treatments, for instance for such diseases as Lyme disease, West Nile fever, malaria, tularemia, plague, typhus and many others. Considering the world-wide presence of stinging and biting insects and the respective frequency of associated diseases, such conventional medical intervention affords a major effort in man-power and financial expenses. There are 30,000 cases of Lyme disease alone reported to the CDC annually (cdc.gov). Preventive measures for immediate treatment of such stings and bites, even by repellents to avoid such stinging insect would be a major advantage for general health care.
Common insect repellents recommended by CDC and EPA (cdc.gov; epa.gov) include DEET (N,N-diethyl-meta-toluamide), IR3535 ((3-[N-butyl-N-acetyl] aminopropionic acid, ethyl ester), Picaridin and a few others.6,7 Such substances, although effective as insect repellent, do not fight infections if a few bites have occurred despite of their use and thus transferred possible infections. It would be a major advantage, therefore, to have a substance which could combine both activities: insect repellent and anti-infectious actions.
We are presenting preliminary data of a study using a newly designed skin protectant cream which combines all three activities (skin protection, repellant, anti-infectious), and thus help to fight secondary infective diseases caused by biting and stinging insect.
Materials and methodsWe used fiteBac Germicidal Hand Softening Gel (GHSG: Fig. 1, kindly provided by KHG fiteBac Technology, 3698 Largent Way, Marietta, GA 30064). The contents of the gel contain two cosmetics: an elastomer (cross linked silicon polymers) as found in lipsticks, antiperspirants, deodorants, and hair products. The second compound is a cosmetic ester PPG (Crodamol) also found in personal care products which combines to the elastomer to form a large polymeric organosilicon compound. The list of ingredient chemicals is as follows: Benzalkonium Chloride, Cyclopentasiloxane, Dimethicone Crosspolymer, PPG-3 Benzyl Ether Ethylhexanoate, Octadecyldimethyl Trimethoxysilylpropyl Ammonium Chloride. The anti-infectious activity of quaternary ammonium salts (QAS) and siloxanes is well documented from its use as polyurethane coating.8–12 The fiteBac Germicidal Hand Softening gel (GHSG), in laboratory testing, showed activities against various bacteria, and suggestive activities against several viruses and fungi (e.g. candida) (13,14[Molinari]) besides its skin cosmetic protectant activities.

This pilot study for an initial screening of GHSG included 23 volunteers with various acute skin disorders (see Table 1), ages 12–81 years, 12 of which were males and 11 females. All consented to participate after respective risk information (“informed consent”).
Clinical data base for GHS (germicidal hand softening) gel treatment.
| Patient (age/sex) | Diagnosis | Cause | Treatment | Result |
|---|---|---|---|---|
| Mosquito bites | ||||
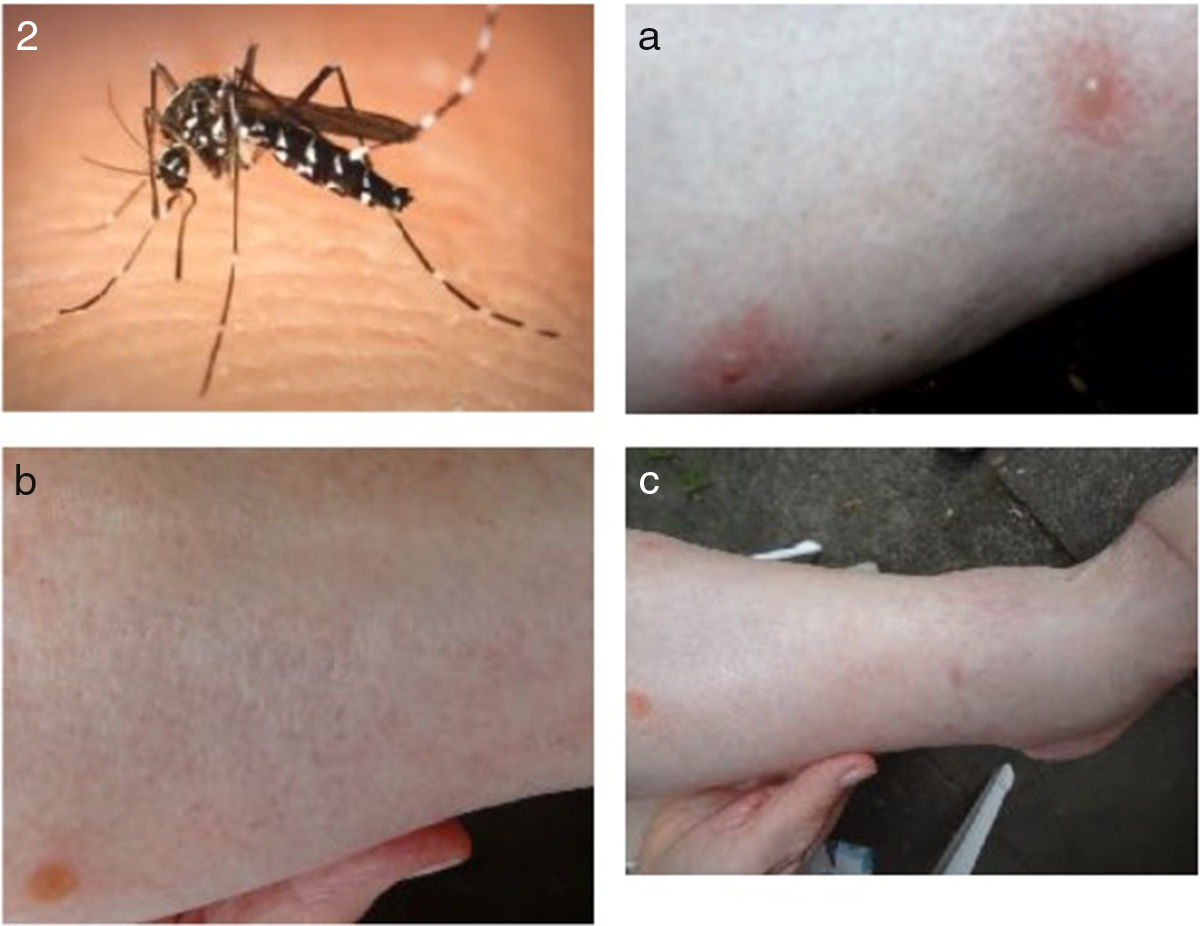
| BK 79/F | Itching flare, edema, epidermal bullae | Chinese tiger mosquito Aedes albopictus (Fig. 2) | GHS for 5 days, one/day | Flare and edema for 2 days drying of bullae, complete resolution 1 week |
| DA 44/M | Erythema, itching | Common mosquito Culex sp. | GHS for 2 days | Complete resolution |
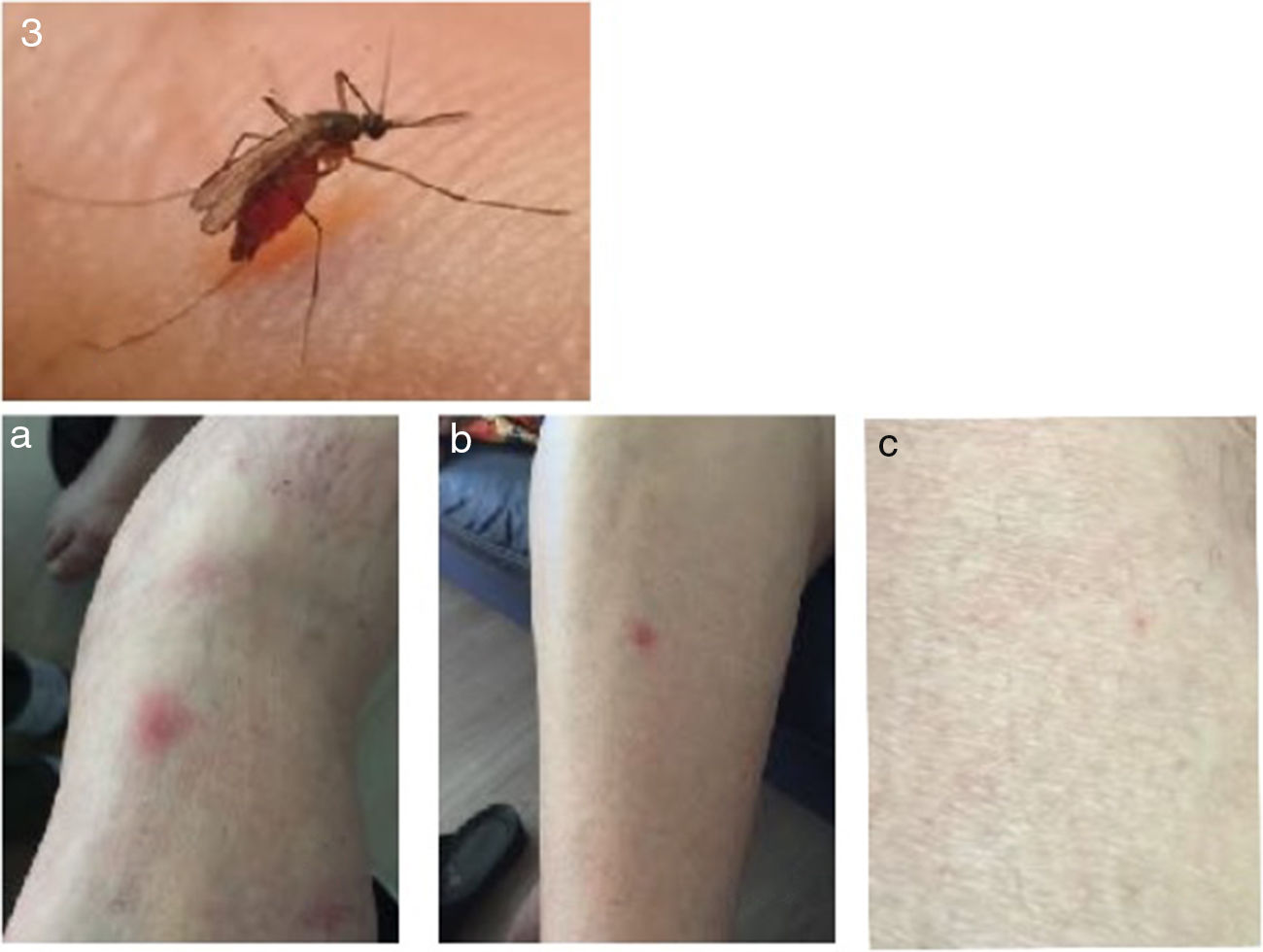
| MBK 81/F | Erythema, itching | Common mosquito Culex sp. (Fig. 3) | GHS for 3 days one/day | Complete resolution |
| GRK 80/M | Erythema, itching | Common mosquito Culex sp. | GHS for 3 days one/day | Complete resolution |
| KN 53/F | Edema, flare, itching | Unidentified mosquito | GHS for 5 days one/day | Complete resolution |
| PF 12/M | Edema, itching, dermal blisters | Chinese tiger mosquito Aedes albopictus | GHS for 3 days twice/day | Complete resolution |
| LMN 23/F | Flare, itching | Unidentified insect | GHS for 4 days one/day | Complete resolution |
| KS 40/M | Mosquito bite prevention | Common mosquito Culex sp. | GHS to arms and legs one/day | Protection |
| DV 18/M | Rash, edema, vesicles | Multiple unidentified mosquitoes | GHS to arms and legs one/day | Resolution in 3 days |
| LN 22/F | Flare, nodule, itching arms and legs | Common mosquito Culex sp. | GHS for 2 days locally on lesions | Resolution |
| Ticks and other | ||||
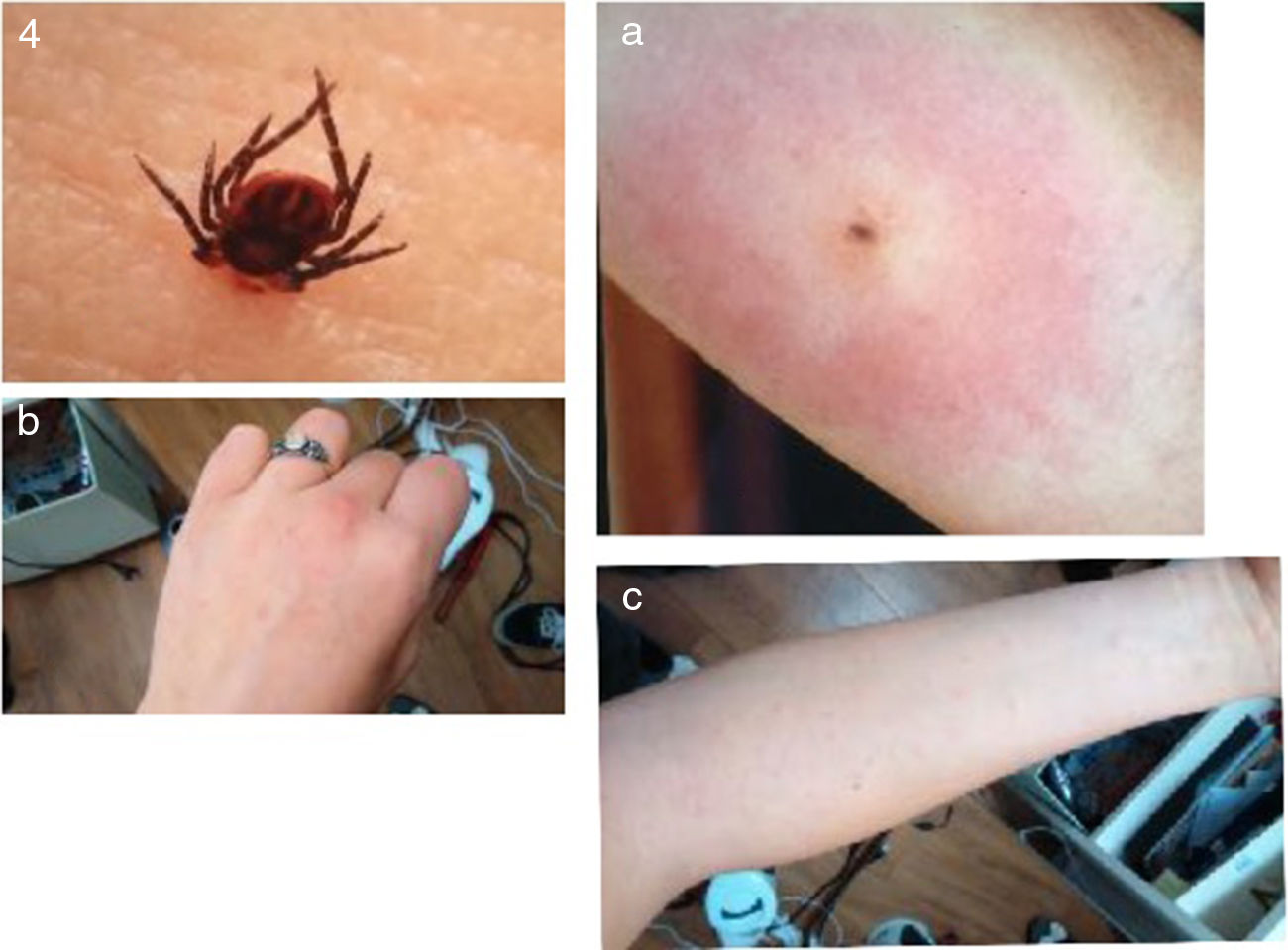
| GK 78/M | Edema, erythema, nodule | Ixodes ricinus (Fig. 4) | GHS for 3 days twice/day | Flare resolved in 2 days nodule in 5 days |
| CN 18/F | Erythema, itching | Unidentified tick | GHS for 6 days one/day | Resolution in 5 days |
| MBK 79/F | Flare, itching, edema blisters | Spider bite (Fig. 5) | GHS for 5 days one/day | Resolution in 1 week |
| Other skin infections | ||||
| RBK 57/M | Edema, local arthritis (finger) | Suspected tick bite | GHS for 4 days ibuprofen creme | Edema, not pain resolution after 2nd week |
| GRFK 80/M | Intertrigo | Suspected candida | GPS for 2 days | Resolution |
| RK 56/M | Rapid growing skin papilloma | Suspected papilloma virus | GPS for 1 week twice/day | Shrinking and disappearance |
| KA 68/F | Onychomycosis finger nails, eczema | Fungus (unidentified) | GHS for 2 weeks resolution | Resolution |
| GK 78/M | Intertrigo | Suspected candida | GHS for 3 days | Resolution |
| LN 21/F | Itchy rash, burning | Suspected neurodermitis GHS for 5 days | Resolution after reddening | Resolution after reddening |
| CSN 51/F | “Dry and choppy hands” | Unidentified | GHS for 1 week | Smooth skin after initial flare |
| GK 76/M | “Fast growing wart” | Suspected papilloma virus | GHS for 1 week | Wart drying in 4 days resolution in 1 week |
| BP 75/F | Intertrigo inframammary crease | Unidentified | GHS for 3 days | Resolution |
| RF 80/M | Intertrigo inguinal | Candida | GHS for 4 days then twice a week | Resolution |
 Mosquito and acute vesicular dermatitis. (b and c) Drying of vesicles and disappearance of lesion after treatment with GHGS.")
 Acute and post-treatment lesion.")
 tick and acute bite.")
 and treatment. Top and (a) spider and acute lesion, (a and b) residual slight skin pigmentation after treatment. Lesion with exanthema migraines. (c) Treatment effects with GHSG.")
The gel was administered to the skin immediately after bites of various insects with early symptoms occurring (reddening, edema, itching, bullous dermatitis). The course of local dermatitis was monitored by photography with follow-up for up to 3 years. Patients were interviewed for eventual late symptoms (fever, head ache, chronic exanthema, arthritis and others). Biting insects were identified – as far as possible – by inspection (see Table 1).
ResultsAll of the 23 cases but one treated with GHS gel reacted positively. Of these, 10 cases lead to complete resolution within 2–3 days. These included acute dermal reactions caused by the common mosquito Culex pipiens; a somewhat delayed reaction in lesions with dermal edema and blisters occurred in bites from the Chinese tiger mosquito, Aedes albopicta also named Stegomyia albopicta (3 days to 5 days). No additional bites were observed after the application of GHS gel for protection of uninvolved skin areas, and no side effects of the gel itself were recorded. One case with several mosquito bites and a 1 day delay in application of the gel afforded 5 days to completely resolve.
Excellent resolution within 2–3 days following GHS gel administration was found in four cases of intertrigo (intertriginous dermatitis, ID). ID develops in skin folds exposed to heat, moisture and friction (e.g. axilla, perineum, inframammary creases and others) and is commonly super-infected by candida organisms or bacteria. Conventional treatment is by drying agents, local antimicobial/antifungal drugs and occasionally topical steroid steroids (personal hygiene notwithstanding and testing for diabetes mellitus).
It took generally longer for complete resolution in cases with tick bites which included more severe local lesions such as blisters, nodular infiltrates, ulceration and – in one case – general exanthema. In such cases, at least one week of local GHS gel administration appeared advised.
Other cases which afforded longer (at least one week) administration included such not clearly identified cases as neurodermitis, certain “warts” (suspicious for papilloma virus infection), and “dry and choppy hands” (in the words of the patient). At least one week of treatment, if necessary longer, were required.
In one case, GHS gel was inefficient to resolve the problem: the patient had a suspected tick bite at the finger (not having identified the tick) with subsequent edema, swelling of the finger, and arthritic pain. After a week's treatment with GHS gel, only the additional application of a local anti-rheumatic ointment (ibuprofen) resulted in complete resolution after a second week.
DiscussionfiteBac Germicidal Hand Softening Gel (GHSG) is available as over-the-counter medication regulated and approved as non-prescription product defined in FDA's Topical Antimicrobial Monograph (RR Stewart, Senior Regulatory Consultant, Technology Science Advisory Group, Washington DC 20036, March 4, 2016). It serves as general skin cosmetic and protectant combined with antimicrobial (bacteria, viruses, certain fungi) activities.13,14 GHSG has several advantages over other preparations commonly used for similar indications. (1) It is a non-alcohol based hand sanitizer thus avoiding negative side effects of alcohols.15–17 It also avoids possible toxic effects of one of its ingredients (benzalkonium chloride) by its embedding in silicon polymers. It reduces resorption of the toxic ingredient significantly18 while protecting the skin and its local microenvironment.
Considering such advantages, we tested GHSG in a pilot study with 23 cases of dermatitis following various insect bites and related conditions. In all but one case, GHSG leads to complete remission of skin pathology caused by insect bites of various kind as well as in 4 cases of intertrigo (a candida- or bacteria-caused dermatitis). The only case in which GHSG was not sufficient was by a delayed application to a tick bite which already had caused arthritic complications. This case also resolved after addition of the anti-rheumatic ibuprofen. Our data thus warrant a greater use of GHSG for treating insect bites and some common dermatitis cases in the elderly.19 No toxic clinical effects were observed clinically during a 3 year period when used as a general cosmetic, and laboratory testing has shown that the gel does not penetrate the skin such as to initiate systemic toxicity.18
Our as well as other data referred to above warrant the tentative use of GHSG against skin infections by candida (e.g. in diabetics, and in babies such as diaper rash), by certain viruses (e.g. papilloma virus “warts” and herpes labialis/genitalis) and possibly to also alleviate the symptoms of shingles. Special targets for using the gel should include nursing homes for the elderly, boys scout- and military camps, as well as for travelers in subtropical and tropical countries.
Besides, GHS gel appears to be useful as insect repellent to avoid biting, and possibly also as general dermal antiseptic especially, as it is not an alcohol-based ointment and it avoids possible toxic side effects of resorbed benzalkonium chloride and common alcoholic preparations.
FundingLocal institutional funding.
Conflict of interestNo conflict of interest for any of the authors.