Postoperative pain after cardiac surgery (CS) can be generated at several foci besides the sternotomy.
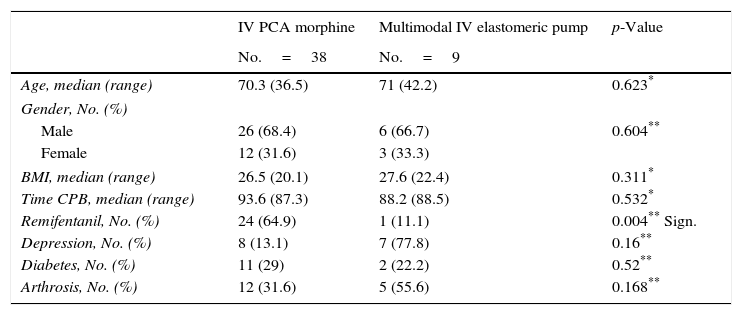
MethodsProspective descriptive longitudinal study on the chronological evolution of pain in 11 sites after CS including consecutive patients submitted to elective CS through sternotomy. The primary endpoints were to establish the main origins of pain, and to describe its chronological evolution during the first postoperative week. Secondary endpoints were to describe pain characteristics in the sternotomy area and to correlate pain intensity with other variables. Numerical Pain Rating Scale from 0 to 10 at rest and at movement on postoperative days 1, 2, 4 and 6. Numerical Pain Rating Scale>3 was considered moderate pain. Statistical analysis consisted in Mann–Whitney U-test, a Chi-squared, a Fisher exact text and Pearson's correlations.
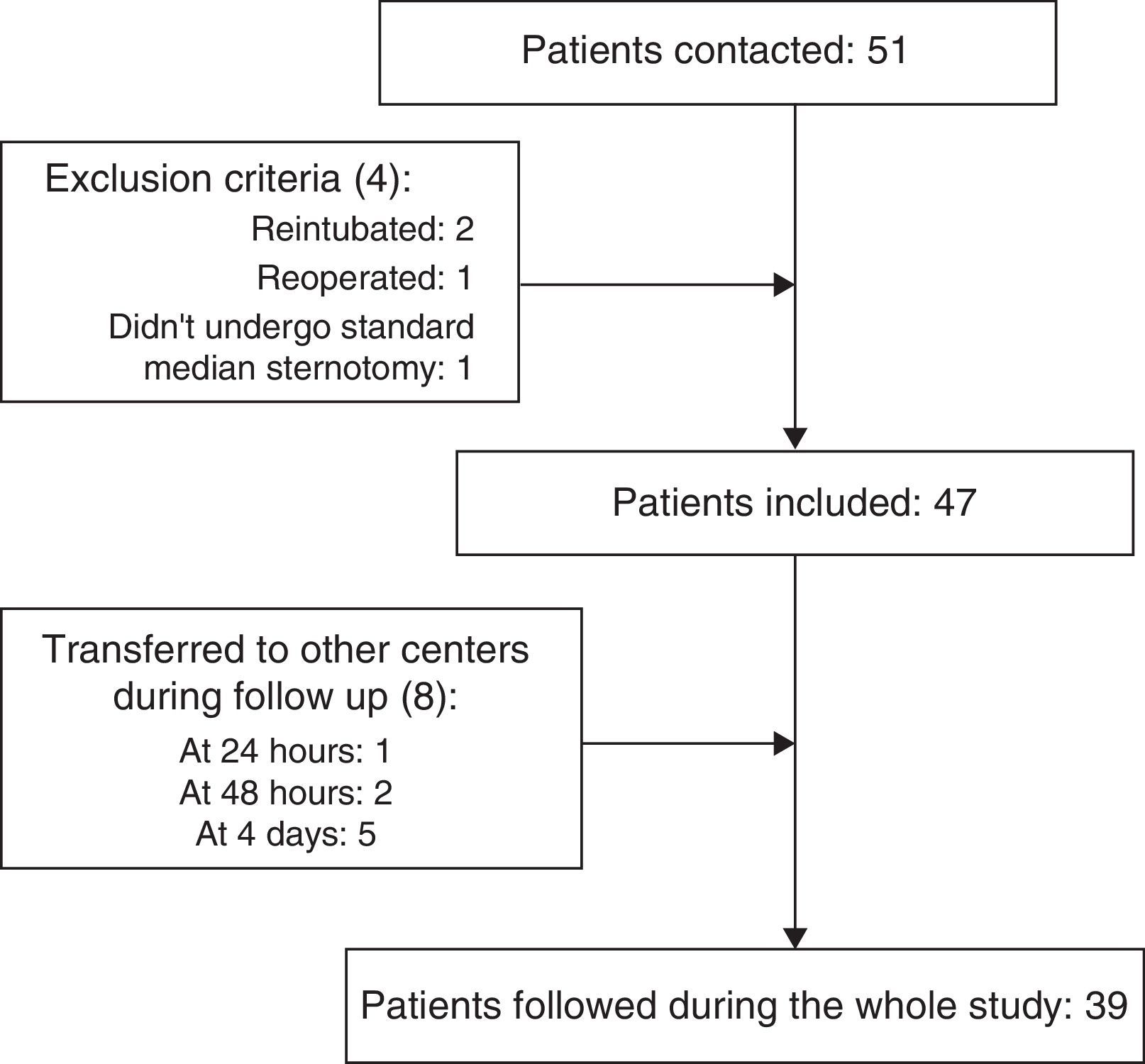
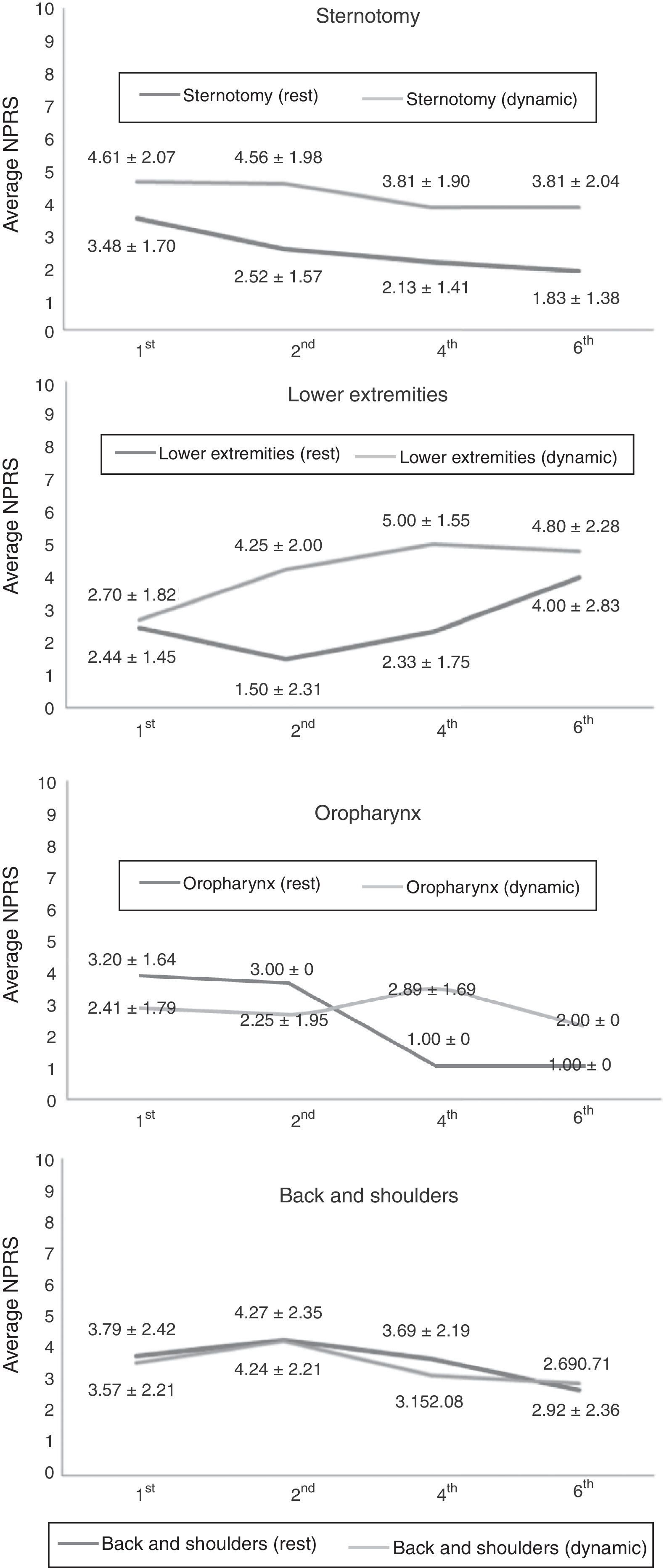
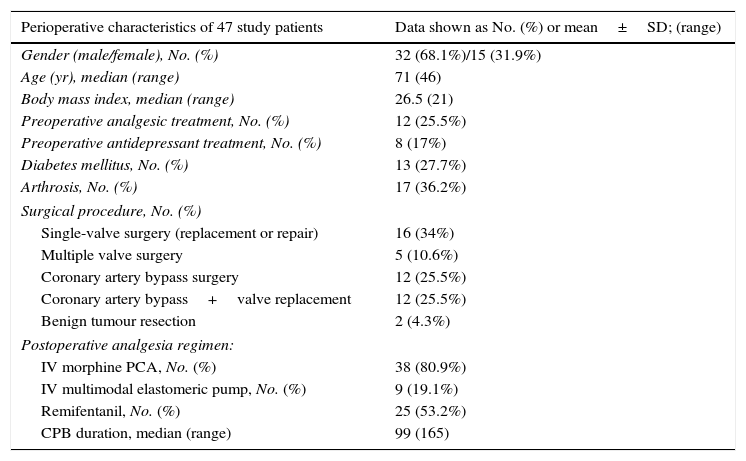
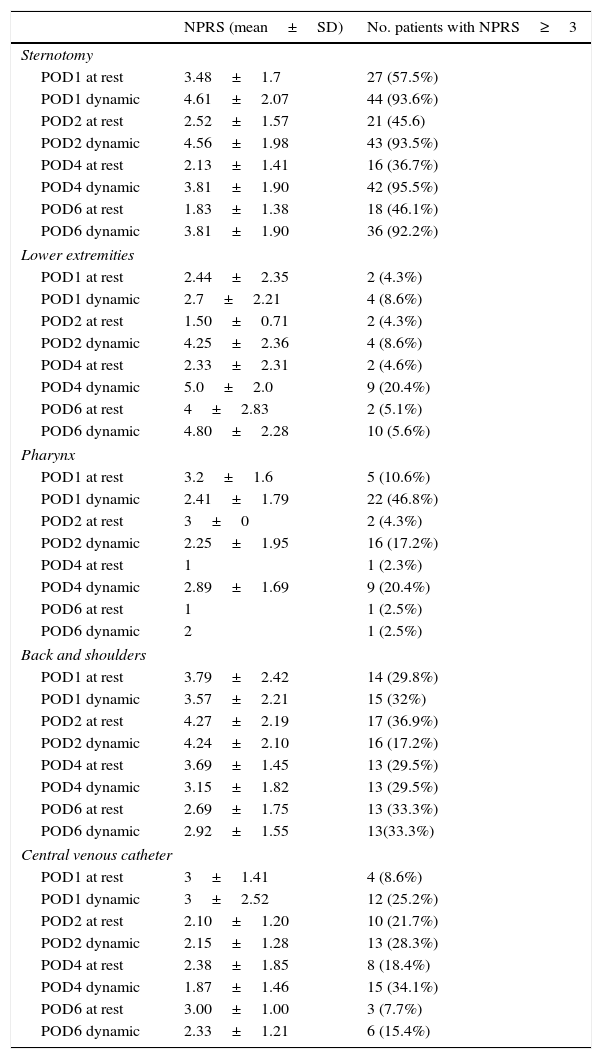
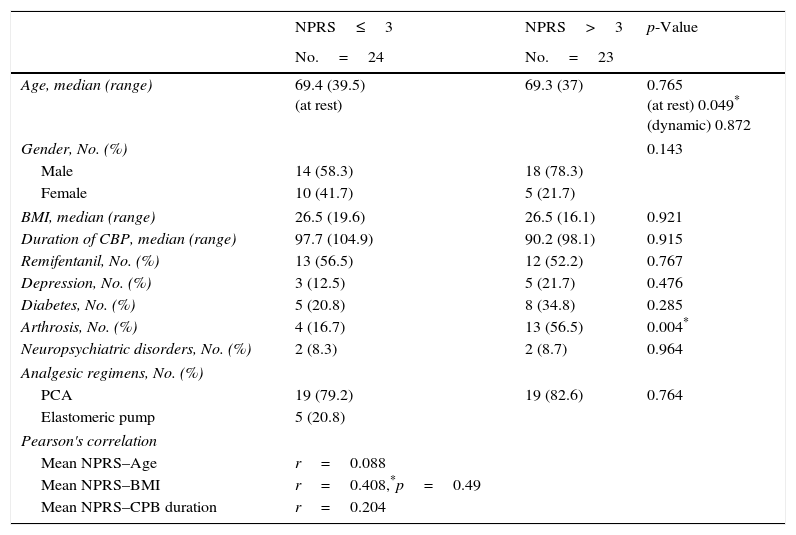
ResultsForty-seven patients were enrolled. In 4 of 11 locations pain was reported as Numerical Pain Rating Scale>3 (sternotomy, oropharynx, saphenectomy and musculoskeletal pain in the back and shoulders). Maximum intensity of pain on postoperative days 1 and 2 was reported in the sternotomy area, while on postoperative days 4 and 6 it was reported at the saphenectomy. Pain at rest and at movement differed considerably in the sternotomy, saphenectomy and oropharynx. Pain at back and shoulders and at central venous catheter entry were not influenced by movement. Pain in the sternotomy was mainly described as oppressive. Patients with arthrosis and younger patients presented higher intensity of pain (p=0.004; p=0.049, respectively).
ConclusionsFour locations were identified as the main sources of pain after CS: sternotomy, oropharynx, saphenectomy, and back and shoulders. Pain in different focuses presented differences in chronologic evolution and was differently influenced by movement.
Tras la cirugía cardiaca (CC) el dolor postoperatorio procede de varios focos, además de la esternotomía.
MétodosEstudio prospectivo, descriptivo y longitudinal sobre la evolución cronológica del dolor en 11 localizaciones tras CC. Se incluyeron pacientes operados consecutivamente de CC por esternotomía. Los objetivos fueron establecer los principales focos del dolor, su evolución cronológica durante la primera semana, correlacionar la intensidad del dolor con otras variables y describir las características del dolor de la esternotomía. Se utilizó la escala de valoración numérica Numerical Pain Rate Scale de 0-10 en reposo y en movimiento en los días postoperatorios 1, 2, 4 y 6. Una puntuación>3 en la Numerical Pain Rate Scale fue considerado dolor moderado. Los datos se sometieron a las pruebas U de Mann-Whitney, Chi cuadrado, exacta de Fisher y la correlación de Pearson.
ResultadosSe incluyeron 47 pacientes. En 4 de las 11 localizaciones del dolor este fue valorado como una puntuación>3 en la Numerical Pain Rate Scale (esternotomía, orofaringe, safenectomía y hombros y espalda). La máxima intensidad de dolor se registró en la esternotomía en los días postoperatorios 1 y 2, mientras que en los días postoperatorios 4 y 6 fue en la safenectomía. El dolor en movimiento fue significativamente mayor que en reposo en la esternotomía, las extremidades inferiores y en la orofaringe. El movimiento no aumentó el dolor en espalda y hombros ni en la entrada del catéter venoso central. El dolor en la esternotomía fue descrito como opresivo. Los pacientes con artrosis y los más jóvenes presentaron dolor más intenso (p=0,049 y p=0,004, respectivamente).
ConclusionesLos principales focos del dolor tras CC fueron la esternotomía, la orofaringe, la safenectomía y el osteoarticular en hombros y espalda. Los focos de dolor mostraron diferente cronología y distinta influencia del movimiento.