



Bone and joint disease has a high incidence and impact on the population. The bone scan is a diagnostic tool that provides important metabolic and clinical information, therefore the interpretation of the images by the nuclear medicine physician must be very precise. The isotopic distribution pattern in hands has not yet been described. For this reason a description is presented of common scintigraphic findings in adults without osteoarticular disease.
Materials and methodsA prospective analysis was conducted on 156 hands of patients whose bone scans met inclusion criteria. There were delineated regions of interest in the carpal, metacarpal, proximal, and distal interphalangeal joints of the second and third fingers of both hands. An analysis was made, including the total counts, means, and standard deviations. The cut-offs were selected using the normal distribution, which was defined as the cut at the 99th percentile of each variable. A semi-quantitative analysis was made of the images.
ResultsThe study included 36 men (23%) and 119 women (77%), and the mean age was 44.9±13.9. The mean total counts gradually decreased from proximal to distal in all age groups and in both genders in the following proportions: the activity in carpus was 4.4 fold more than the metacarpus; the metacarpus was 1.7 fold more than proximal interphalangeal joint; proximal interphalangeal joint was 1.4 fold more than distal one.
ConclusionsA scintigraphic pattern consisting of a gradual decrease from proximal to distal joints (degradation) was found in the hands of adults without bone and joint disease, regardless of gender and age.
La gammagrafia ósea es uno de los estudios más frecuentemente utilizados para el abordaje diagnóstico de la patología osteoarticular, sin embargo, no se conocen patrones claros de normalidad para algunos sitios anatómicos, llevando a tasas altas de variabilidad interobservador, como es el caso de la evaluación de las manos. No se encuentra en la literatura una descripción del patrón gammagráfico normal sobre manos, por lo cual pretendemos describir el patrón de captación más frecuente en una población adulta sin enfermedad osteoarticular.
Materiales y métodosSe hizo un análisis prospectivo de 156 gammagrafías óseas sobre manos que cumplieron el criterio de inclusión. Se delinearon regiones de interés en el carpo, metacarpo, articulaciones interfalángicas proximales y distales de los dedos índice y medio de ambas manos; se tomaron las cuentas totales, se analizaron promedios y desviación estándar, y se hizo análisis semicuantitativo de la imagen.
ResultadosSe incluyeron 36 hombres (23%) y 119 mujeres (77%), la edad media fue de 44.9±13.9. Los promedios de las cuentas totales disminuyeron progresivamente de proximal a distal en todos los grupos de edad y en ambos géneros, siguiendo la siguiente proporción: carpo 4.4 veces más que metacarpo; metacarpo 1.7 veces más que interfalángica proximal; interfalángica proximal 1.4 veces más que distal.
ConclusionesEn manos de pacientes adultos, sin enfermedad osteoarticular, sin distinción de género y edad, encontramos un patrón gammagráfico en «degradé» con mayor concentración isotópica en carpo, seguida del metacarpo y de las articulaciones interfalángicas proximales y distales.
During the last decades, nuclear medicine studies have demonstrated an accelerated growth, due to the development of new and better radiopharmaceuticals1–3; among the numerous isotopic studies, bone scintigraphy is the second most frequently performed procedure in the nuclear medicine services4,5 after myocardial perfusion; only in the United States, more than 3,450,000 of these procedures were carried out in the year 2005, being the inflammatory and osteoarticular pathology one of the most important indications.4,6
In the study of the osteoarticular pathology (degenerative/inflammatory) of the hand, nonisotopic images play an important role, being conventional radiography the simplest, most economical and widely used method, especially in the initial assessment.7,8 Another important technique is the nuclear magnetic resonance which evaluates early changes in the articular cartilage before bone destruction occurs.9,10 On the other hand, ultrasonography is used to evaluate joint effusions and erosions, and currently there are stratification systems such as Power Doppler, which has demonstrated to be reproducible and accurate for synovitis of the hand.11–13
The bone scan is not part of the initial evaluation of osteoarticular disease, but is highly sensitive to detect changes previous to structural alterations, it is also reproducible and it has a negative predictive value higher than 90%14,15; it can help to discriminate the origin of the pain (soft tissues or bone), locate the most painful points in patients with complex symptoms16,17 and detect bone pathologies when other imaging techniques have failed.18 The radiopharmaceutical most commonly used for bone imaging is methylene diphosphonate which, bound to Tc99m forms a radioactive compound which reaches the bone through the bloodstream and binds to hydroxyapatite crystal with high affinity,19,20 allowing to evaluate indirectly the osteoblastic activity.
The identification and the familiarization with the normal pattern of radiotracer uptake in the hands are very important for the proper scintigraphic evaluation of this area; however, at the present time there is no recognized normal scintigraphic reference pattern. Making a review of the literature, it was found only one study related to the subject, conducted by Wilfrido et al., who in 1977 mentioned in a heterogeneous group of patients some normal trends of radiotracer concentration, divided into 2 groups, the first with a detailed image of the joints of the hand seen in adolescents, and the second, in a pattern called “washed-out” with less definition of the image, observed in older patients.21
Knowing the normal patterns of radiotracer concentration in the different bone structures allows to improve the diagnostic accuracy, avoiding overdiagnoses and underdiagnoses.
The purpose of this study is to describe the radiotracer distribution pattern in the bone scan of the hands of adult patients without osteoarticular pathology, under a semi-quantitative analysis which can be reproducible and that allows and objective evaluation of the hands.
Materials and methodsPatientsIn the study were included 156 hands of patients (36 men, 119 women) between 18 and 72 years old, referred between November 2012 and November 2013, to the Nuclear Medicine Service for a bone scan to study oncological or maxillofacial pathology, who to interrogation did not report antecedents of osteoarticular disease of degenerative or rheumatic inflammatory type, previous surgeries, metabolic bone disease, plegias or stress injuries; the images were taken from the records of patients of the Nuclear Medicine Service of the Colsanitas Clinics in Bogota (Colombia Clinic and Reina Sofia Clinic) and the antecedents were verified in the respective medical histories. The selection of the participants was made by convenience, based on the records of hands accomplished in the Nuclear Medicine Service.
RadiopharmaceuticalTc99m-MDP was used; the administered dose was 20mCi (740MBq) and it was injected in a peripheral vein in the foot.
Scintigraphic imagesThe studies were acquired by a double-headed gamma camera with a high resolution collimator, GE Infinia, coupled to an Odysey VP workstation, using the Xeleris Functional Imaging, bone evolution software. A 3-phase bone scan with special approach to the hands (in the 3 phases) was performed acquiring perfusion images during one minute (one frame/3s) in a matrix of 64×64 on the hands, the image of the tissue distribution was obtained 5min after the injection of the radiopharmaceutical (tissue phase) in a matrix of 128×128, and 3h post-injection were obtained images in a matrix of 128×128, with a number of 500,000 counts per image for the bone phase.22 Only the images of the bone phase were taken into account for the semi-quantitative analysis.
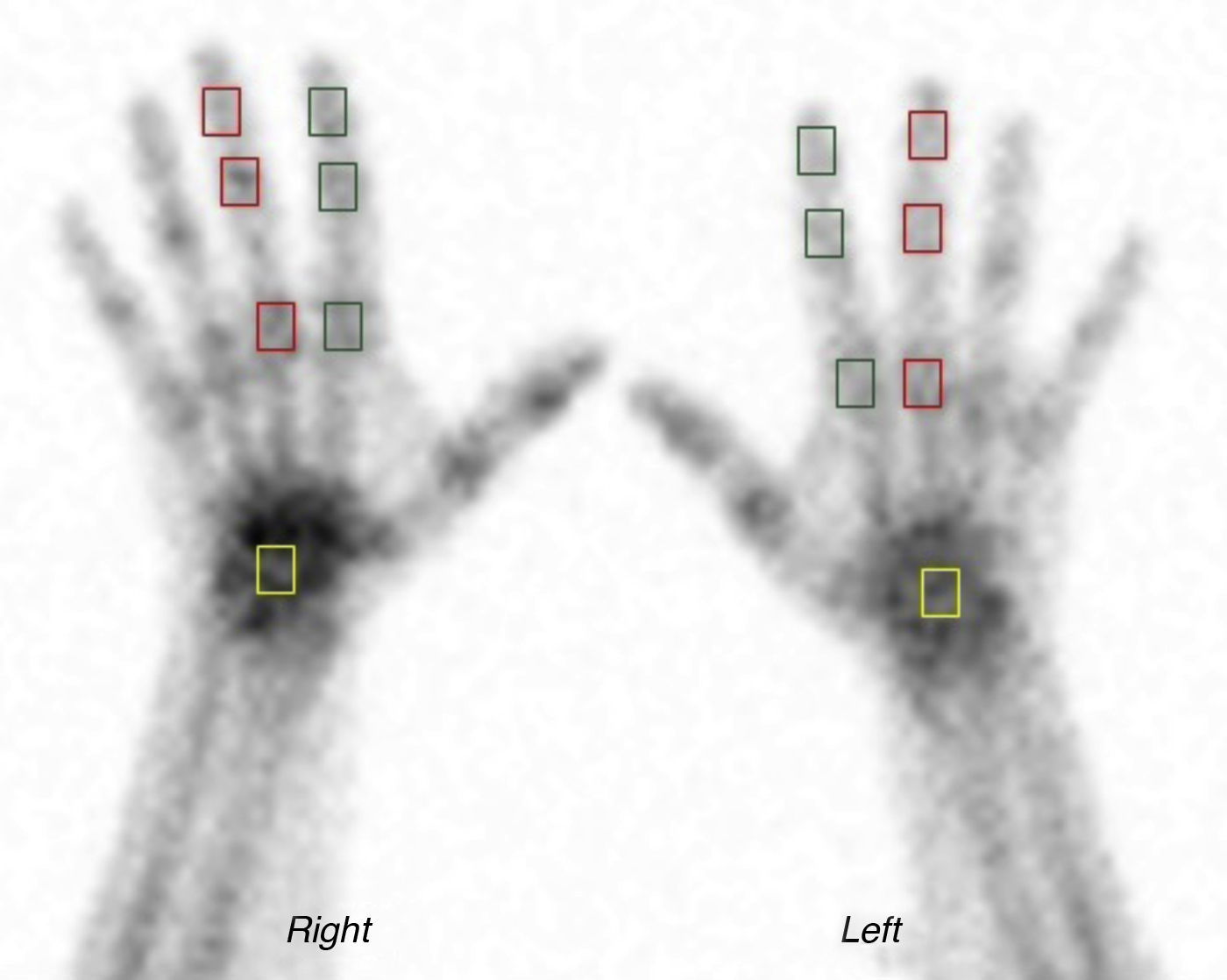
Analysis of the imagesRegions of interest (ROI) of the same size were delineated on the carpus and the metacarpophalangeal and proximal and distal interphalangeal regions of the index (called finger 1 for the analysis) and middle (called finger 2 for the analysis) fingers, obtaining total counts in order to analyze their trends and compare them each other (Fig. 1).

Areas of interest. Bone scintigraphy of the hands; in green squares, areas of interest on the interphalangeal and metacarpophalangeal joints of the second finger; in red squares, areas of interest on the interphalangeal and metacarpophalangeal joints of the third finger; in yellow squares, areas of interest on the carpus.
The data were analyzed according to gender and age, for which the population was grouped as follows: 18–25, 26–35, 36–45, 46–55, 56–65 and older than 65 years.
The mean total counts, proportion ratios, mean and standard deviation were used for the statistical analysis, and their behavior in each variable was analyzed; p<0.05 was considered significant. The normality of each of the variables analyzed was evaluated using the Shapiro–Wilk test and the null normality hypothesis of normality was rejected with p<0.05. A bivariate analysis comparing the qualitative variables by gender was carried out using the Wilcoxon Rank sum test; and the analysis of each variable by age groups was performed using the Kruskall–Wallis test.
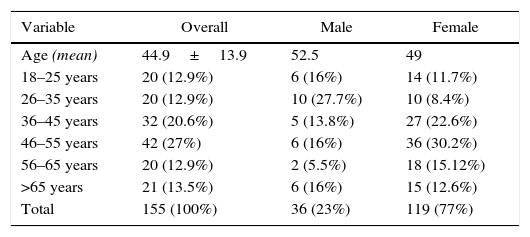
ResultsThe hands analyzed corresponded to 155 patients, the overall average age was 44.9 years, 52.5 years for men and 49 years for women. The age group with the highest representation in this series of patients was the one of 46–55 years. The series is represented in 23% by men and 77% by women (Table 1).
Population characteristics.
| Variable | Overall | Male | Female |
|---|---|---|---|
| Age (mean) | 44.9±13.9 | 52.5 | 49 |
| 18–25 years | 20 (12.9%) | 6 (16%) | 14 (11.7%) |
| 26–35 years | 20 (12.9%) | 10 (27.7%) | 10 (8.4%) |
| 36–45 years | 32 (20.6%) | 5 (13.8%) | 27 (22.6%) |
| 46–55 years | 42 (27%) | 6 (16%) | 36 (30.2%) |
| 56–65 years | 20 (12.9%) | 2 (5.5%) | 18 (15.12%) |
| >65 years | 21 (13.5%) | 6 (16%) | 15 (12.6%) |
| Total | 155 (100%) | 36 (23%) | 119 (77%) |
The mean total counts from the carpus to the distal interphalangeal joints of the index and middle fingers, which were analyzed as a reference point, gradually decreased in all age groups; it was only found a difference in the counts of the carpus in the groups of 46–55 years and >65 years with regard to the other groups.
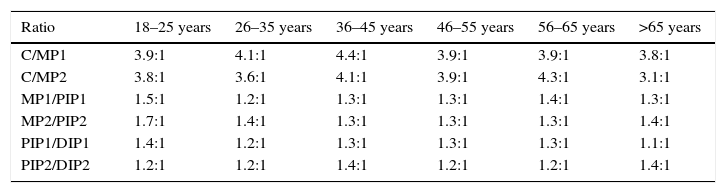
The proportion ratios between the different studied joints and in all age groups (carpus/metacarpophalangeal and proximal interphalangeal/distal interphalangeal in both hands) are shown in Table 2.
Ratios by age group.
| Ratio | 18–25 years | 26–35 years | 36–45 years | 46–55 years | 56–65 years | >65 years |
|---|---|---|---|---|---|---|
| C/MP1 | 3.9:1 | 4.1:1 | 4.4:1 | 3.9:1 | 3.9:1 | 3.8:1 |
| C/MP2 | 3.8:1 | 3.6:1 | 4.1:1 | 3.9:1 | 4.3:1 | 3.1:1 |
| MP1/PIP1 | 1.5:1 | 1.2:1 | 1.3:1 | 1.3:1 | 1.4:1 | 1.3:1 |
| MP2/PIP2 | 1.7:1 | 1.4:1 | 1.3:1 | 1.3:1 | 1.3:1 | 1.4:1 |
| PIP1/DIP1 | 1.4:1 | 1.2:1 | 1.3:1 | 1.3:1 | 1.3:1 | 1.1:1 |
| PIP2/DIP2 | 1.2:1 | 1.2:1 | 1.4:1 | 1.2:1 | 1.2:1 | 1.4:1 |
DIP1: distal interphalangeal finger 1; DIP2: distal interphalangeal finger 2; PIP1: proximal interphalangeal finger 1; PIP2: proximal interphalangeal finger 2; MP1: metacarpophalangeal finger 1; MP2: metacarpophalangeal finger 2.
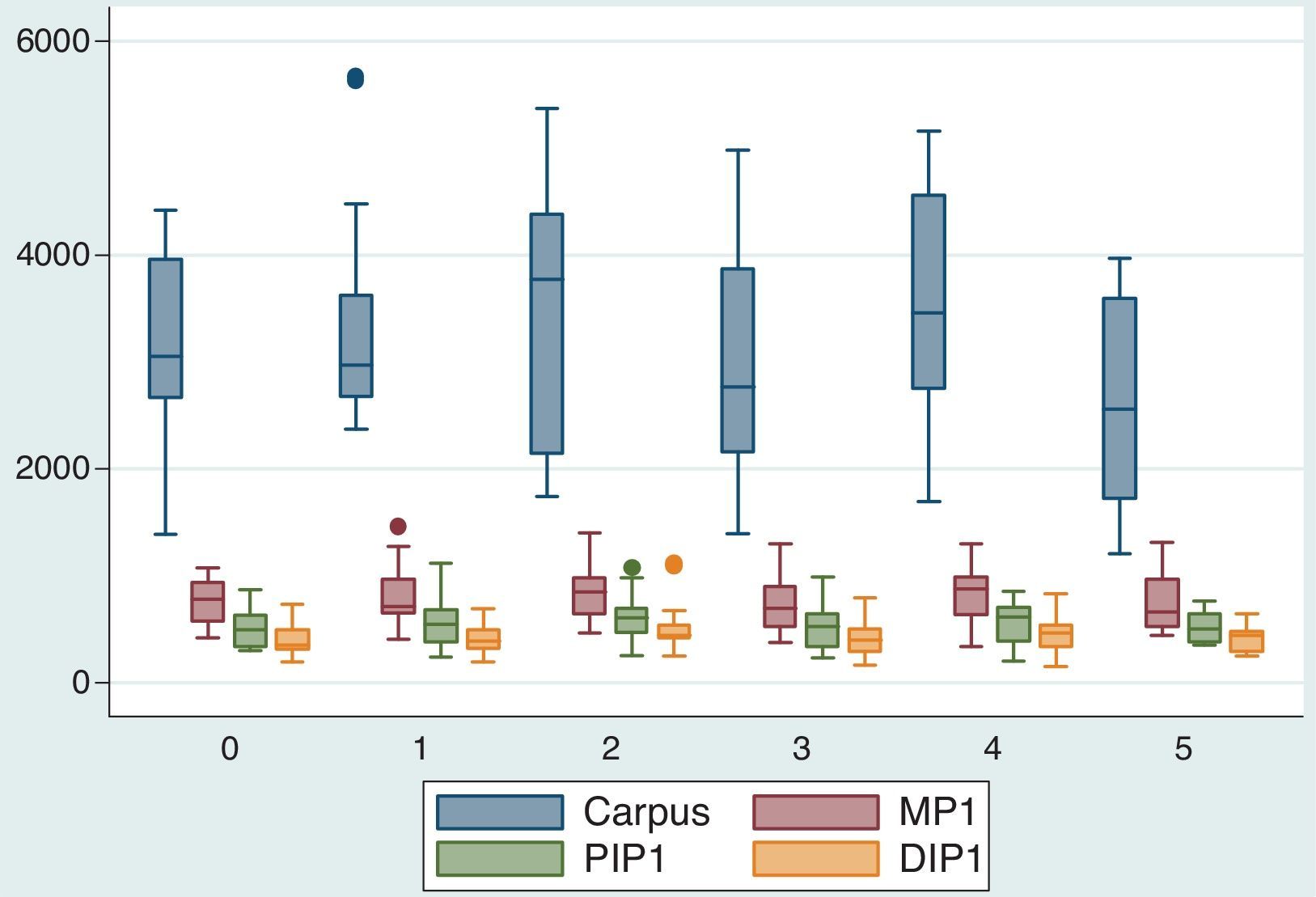
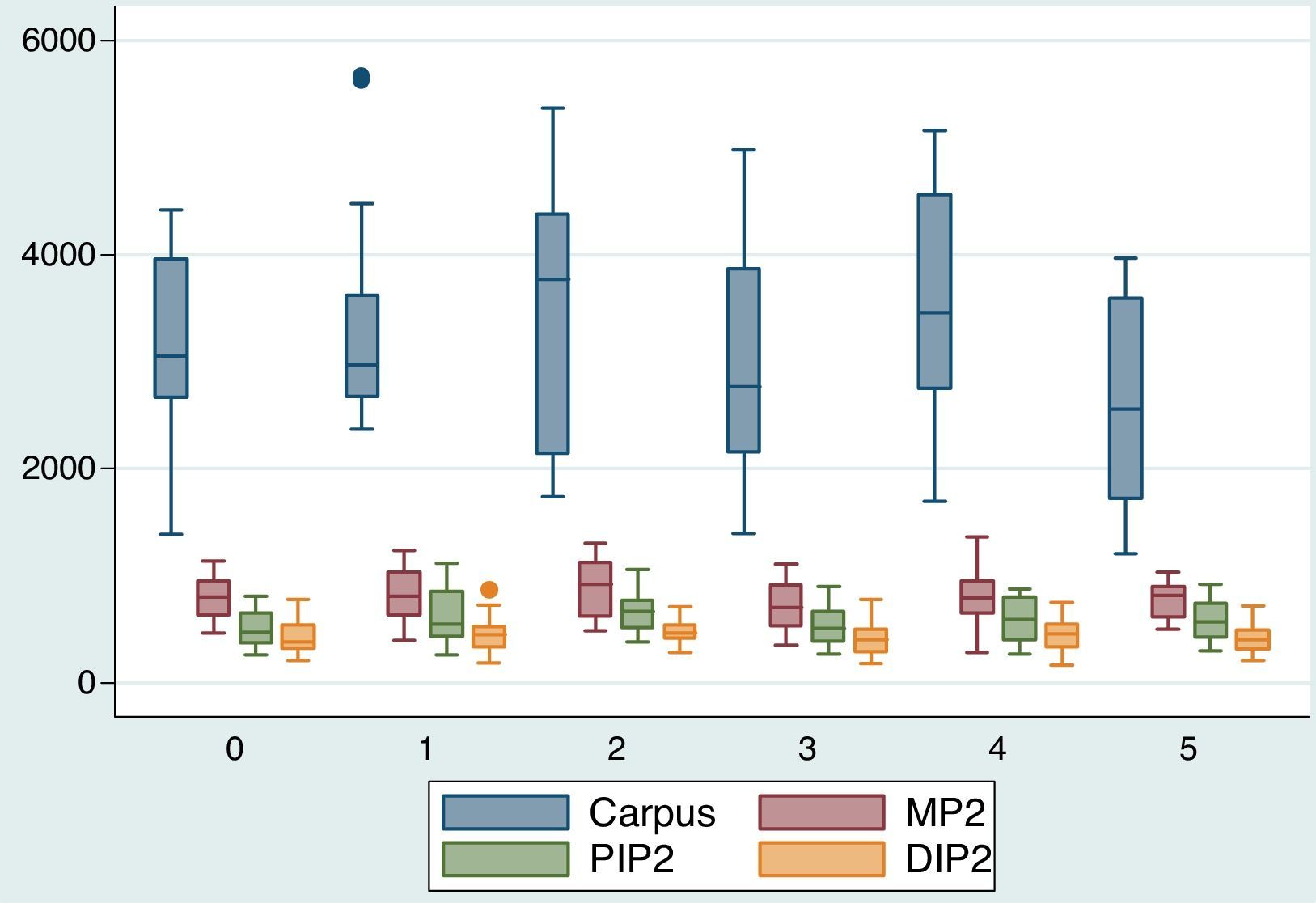
The trends of the means by age group in the different joints in which the ROIs were taken were similar (Figs. 2 and 3). A proximal to distal decrease of the counts was observed as mentioned above.
.")
.")
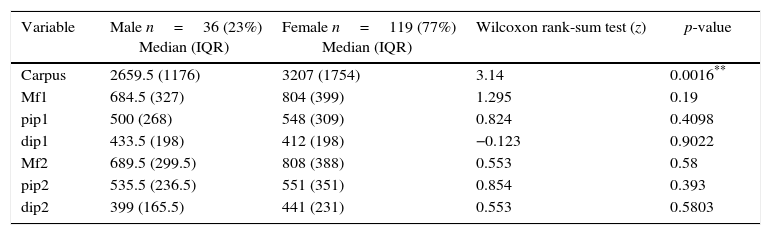
According to the gender, the median of the counts gradually decreased from proximal to distal in all joints, and without distinctions; the mean of the counts of the carpus was higher in women (Table 3).
Description of the median of the counts by gender.
| Variable | Male n=36 (23%) Median (IQR) | Female n=119 (77%) Median (IQR) | Wilcoxon rank-sum test (z) | p-value |
|---|---|---|---|---|
| Carpus | 2659.5 (1176) | 3207 (1754) | 3.14 | 0.0016** |
| Mf1 | 684.5 (327) | 804 (399) | 1.295 | 0.19 |
| pip1 | 500 (268) | 548 (309) | 0.824 | 0.4098 |
| dip1 | 433.5 (198) | 412 (198) | −0.123 | 0.9022 |
| Mf2 | 689.5 (299.5) | 808 (388) | 0.553 | 0.58 |
| pip2 | 535.5 (236.5) | 551 (351) | 0.854 | 0.393 |
| dip2 | 399 (165.5) | 441 (231) | 0.553 | 0.5803 |
DIP1: distal interphalangeal finger 1; DIP2: distal interphalangeal finger 2; PIP1: proximal interphalangeal finger 1; PIP2: proximal interphalangeal finger 2; MP1: metacarpophalangeal finger 1; MP2: metacarpophalangeal finger 2.
We observed in our series that the mean of total counts registered in each of the regions of interest showed a similar trend in all age groups and genders, finding the largest number of counts in carpi, followed by the metacarpophalangeal and the proximal and distal interphalangeal joints, respectively.
In the analysis of counts of the ROIs in the carpus, statistically significant differences were found in the groups of 35–45 years and older than 65 years, finding in the latter a smaller number of counts, explained probably by the physiologically decreased bone metabolic activity. Nevertheless, the trend and the relationship between the counts of the carpus and the metacarpophalangeal joints in these age groups was preserved; likewise, when the ROIs of the same joint were compared between genders, we found greater activity in the carpi of the hands of women with respect to men, a finding that could have been affected by a greater female population in the sample (77%).
The qualitative analysis of the characteristics of uptake was supported by the semi-quantitative analysis and we can say that the pattern is characterized by a progressive decrease in the concentration of the radiotracer that goes from proximal to distal and that we call “degradation”. We also observed how the carpus was the region of interest of the hand with greater activity with an uptake of up to 4.4 folds more in relation with the metacarpophalangeal joint; the proportion ratios found demonstrate this behavior and also allow us to see how in the different age groups the metacarpophalangeal joint also shows and increase in the tracer uptake of up to 1.7 folds more than the proximal interphalangeal joint and this in turn concentrates up to 1.4 folds more than its adjacent distal interphalangeal joint, being this finding another way to describe the degradation pattern previously described.
It should be mentioned that the osteoarticular pathology of the hand has received relatively little attention compared with other structures such as the hip of the knee, however, it causes significant disability and deterioration in the quality of life23,24; in osteoarticular disease the involvement of the hands is frequent and it can be made a clinical approach to the origin of the pathology depending on the location of the affected areas, for example, the commitment of the distal interphalangeal and the trapezium-metacarpal joints guides toward a degenerative origin,25 in rheumatoid arthritis the involvement is predominantly in the metacarpophalangeal joints with frequent tenosynovitis of the flexor and extensor apparatus.26,27
The different diagnostic tools allow us to get closer to the understanding of these entities, the simple radiography is used both in the initial assessment and in the evaluation of the severity and follow-up; it has the disadvantage that small variations in the position of the hand during its acquisition can simulate or mask lesions.7 Nuclear magnetic resonance is being increasingly used, especially with techniques that use contrast media such as gadolinium, improving the specificity of the study; however, it requires a suitable and reproducible protocol, in addition to being limited in the presence of osteosynthesis materials.28,29
The bone scan of the hand is a very useful tool with great potential to provide accurate information to the clinician, given its high sensitivity and reproducibility, but a clear normal pattern is not available; this situation demonstrates why the interpretation of our studies must be based on a detailed analysis, in such a way that it will not generate wrong diagnoses. In the literature there are not studies that demonstrate the normal behavior of the joints of the hand under the nuclear medicine metabolic viewpoint, being this study, to our knowledge, the first of its kind; abnormal scintigraphic patterns such as focal hyper-uptake in the distal interphalangeal, scaphotrapezial and the first carpometacarpal joints have been reported in patients with nodal osteoarthritis,30 as well as diffuse hyper-uptakes in the carpus of patients with psoriatic and rheumatoid arthritis, however, without taking into account a basal normality pattern.31
Our study allowed us to know the scintigraphic pattern on the hands in terms of the relationship between each of the joints, however, we did not analyzed the maximum allowed ranges in each of them and we believe that it may be a subject for further studies. Likewise, it may be interesting to analyze in larger samples and with equal representative groups for each gender, is this trend is preserved and to present more accurately the model of “degradation” as a synonymous with normality.
ConclusionsOsteoarticular pathology is part of the most frequent reasons of consultation in the nuclear medicine units. This study is the first that analyzes in a detailed way the behavior of the hands in a bone scan from the qualitative and semi-quantitative viewpoints. Being the hands a frequent site of commitment in degenerative and inflammatory pathology, we believe that the description of a normal pattern called by us “degradation” becomes a tool of great usefulness for medical practice.
Study approved by the Ethics Committee of the Faculty of Medicine of the Sanitas University Foundation.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingResources from the Medical Imaging research group of the Sanitas University Foundation.
Conflict of interestThe authors declare they do not have any conflict of interest.
Please cite this article as: Fuentes LKA, Germán GHC, Niño ME. Hallazgos gammagráficos en manos de población adulta, sin patología osteoarticular, bajo un análisis semicuantitativo. Rev Colomb Reumatol. 2017;24:25–31.
