



In patients with haemophilia, quality of life can be affected by factors like arthropathy, age, and pain intensity.
ObjectiveTo evaluate the health-related quality of life in patients with haemophilia in Medellin during 2014.
Patients and methodsAn observational, descriptive, cross-sectional study was conducted on 60 patients with confirmed diagnosis of haemophilia. Demographic, clinical and lifestyle characteristics are described. Functional test were performed including measuring ranges of mobility and the six-minute walk test. The health-related quality of life (SF-36 and KIDSCREEN-27), disability (WHODAS II), pain (VAS), and depressive symptoms (PHQ-9) were also evaluated.
ResultsA total of 59 patients agreed to participate in the study. The mean age was 28 years (SD ±14.8), with mild haemophilia in 5%, moderate haemophilia in 20.3%, and severe haemophilia in 74.5%. Almost all (96.6%) of the patients were under treatment with prophylaxis, and 84% of the patients were having physiotherapy. The main comorbidity was haemophilic arthropathy in 71% of cases, followed by dyslipidaemia (27%), overweight (20%), and smoking (11.8%). The six-minute walk test reported mean distance of 584.2m, and the SF-36 scores were similar to the general population.
ConclusionThis group of patients with haemophilia reported a quality of life as high as the general population in Colombia without haemophilia. This finding reiterated the importance of the treatment with prophylaxis and the active participation of patients in a rehabilitation program, which promotes functional independence and a healthy lifestyle.
En pacientes con hemofilia la calidad de vida se puede afectar por factores como la artropatía, edad e intensidad del dolor.
ObjetivoEvaluar la calidad de vida relacionada con la salud en personas con hemofilia, en Medellín durante 2014.
Pacientes y métodosEstudio descriptivo observacional de corte trasversal, realizado en 60 pacientes con hemofilia. Se describen las características demográficas, clínicas y de estilo de vida. Se realizó prueba funcional con medición de arcos de movilidad y test de marcha de 6 min, medición de calidad de vida relacionada con la salud (SF-36 y KIDSCREEN-27), evaluación de discapacidad (WHODAS II), dolor (EAV) y síntomas de depresión (PHQ-9).
ResultadosCincuenta y nueve pacientes aceptaron participar en el estudio, edad promedio de 28 (SD±14.8) años, hemofilia leve 5%, moderada 20.3% y grave 74.5%. El 96.6% estaba en tratamiento con profilaxis y el 84% de los pacientes asistía a terapia física. La mayor comorbilidad fue artropatía hemofílica en el 71% de las personas, seguida de dislipidemia (27%), sobrepeso (20%) y tabaquismo (11.8%). La prueba de marcha reportó una distancia promedio de 584.2 metros y los puntajes del SF-36 fueron similares a los de la población general.
ConclusiónEste grupo de pacientes con hemofilia, reporta una calidad de vida tan alta como la población general colombiana sin hemofilia. Este hallazgo reitera la importancia del tratamiento con profilaxis y de la participación activa de los pacientes en un programa de rehabilitación que promueva la independencia funcional y un estilo de vida saludable.
Life expectancy is increasing in people with haemophilia, a disease of genetic origin which is autosomal recessive linked to the X chromosome, whose main manifestation is the hemorrhage, which can occur in any anatomic site, although the most common locations are the muscles and joints. According to the deficient factor it can be classified as A (factor VIII) or B (factor IX) and, according to the levels of the deficient factor, is classified into: mild (5–40%), moderate (1–5%) and severe (<1%).1 In Colombia, the prevalence in men and women is 3.8 cases per 100,000 inhabitants, which makes it an orphan disease, and according to the records of the Ministry of Health and Social Protection, 1525 cases of haemophilia A and 307 cases of haemophilia B are reported.2
As longevity increases, the expectations of living with fewer sequels of the disease to be able to enjoy life, with a functionality that allows the individual to be independent in the activities of daily living and to participate in the family and social environments also increase. Thus, the evaluation of the health status of these patients, has moved to an emphasis in the health outcomes based on the patient's perception of his illness, in accordance with the concept of health-related quality of life (HRQoL),3 understood as a multidimensional construct that takes into account the physical, emotional, mental (cognitive), social and behavioral aspects of the well-being and the functioning (mobility) of the individual, as perceived by himself or by his observers.
In previous studies have been described some factors that could influence the HRQoL in people with haemophilia such as: age, pain intensity, severity of the haemophilia, decreased ranges of motion in the major joints, presence of inhibitor, body mass index, educational level and marital status. Some factors that improve the quality of life (QL) are: pharmacological prophylaxis started at an early stage in order to prevent hemorrhages in patients with moderate-severe haemophilia and, thus, prevent or minimize the damage; participation in a rehabilitation program through exercise, orthesis, physical and occupational therapy, and orthopedic surgical interventions for the control of bleeding through radioactive synoviorthesis or synovectomy, and also correct articular deformities with osteotomies, tendon lengthening or arthroplasties.4,5
The objective of this study was to describe the HRQoL in a group of patients with haemophilia and compare it with that of the general population of Colombia.
Materials and methodsSubjectsAn observational, descriptive, cross-sectional study was conducted in a sample of 60 patients with confirmed diagnosis of haemophilia, who received treatment in the Institution INTEGRAL IPS, haemophilia treatment center, in Medellin (Colombia) in the year 2014.
The eligibility criteria were: patients with confirmed diagnosis of haemophilia who were under treatment in INTEGRAL IPS in the year 2014, accepted to participate in the study and signed the informed consent. The exclusion criteria were: not speaking Spanish, or a neurological alteration that would prevent the filling out of the scales. The study was approved by the scientific committee of INTEGRAL IPS.
Evaluation proceduresFor a clinical and demographic characterization, the following data were obtained: age (years), weight (kg), height (m), type of haemophilia (classified as A or B), severity (classified according to the level of the deficient factor: mild, moderate and severe), treatment (prophylaxis or on-demand), presence or absence of inhibitors, infections with hepatitis B, hepatitis C, human immunodeficiency viruses, comorbidities (diabetes, arterial hypertension, heart disease and articular lesions). According to their occupation, the patients were divided into: younger than 2 years, students, employed, unemployed, or pensioners.
The following variables were also analyzed: physical therapy (attendance to the program of physical therapy reported by the patient as the number of sessions per week in the last month), sports activity (physical activity reported by the patient, outside working hours, during at least 30min, 3 or more times per week during the last month) and the use of walking aids (walking stick, walker, crutches).
It was determined the presence of cardiovascular risk factors: overweight (body mass index ≥25, and obesity, body mass index ≥30), smoking (the patients who reported smoking one or more cigarettes per day at the time of the interview were considered as smokers) and consumption of abuse substances in the last month (defined by the World Health Organization as any substance that, introduced into the body by any route of administration, produces in some way an alteration of the natural functioning of the central nervous system of the individual and, in addition, is susceptible to create dependency, either psychological, physical, or both).
For the measurement of the motion ranges in this study, the shoulder, elbow, knee, hip and ankle were called major joints. The patient was asked to tell which joint(s) limited him most in the activities of daily living, regardless of whether or not it was painful. In this joint(s), the passive arches of flexion and extension were measured by means of a manual goniometer. The deficit of the motion range in the individual movement was obtained from the difference between the normal motion range minus the motion range found in the patient. The deficit of the motion range of the individual movement was reported as a positive value. For example, in a patient with disability for the full knee extension, the angle would be 0°−(−30°)=30°, according with the technique reported by Chen et al.5 In order to make an interpretation based on the function, it was decided to analyze in the upper limbs the flexion deficit, since the functional patterns of the hands are accomplished mainly with flexion of the elbow and the shoulder. In the lower limbs it was decided to analyze the extension deficit because it limits the gait function.
The function was also evaluated with the 6-min walk test, which is a test that allows to estimate the functional capacity and is performed asking the patient to walk at the highest speed possible without causing pain, continuously during six minutes, in a track that measures between 25 and 30m. The interpretation was made based on the distance walked in meters.6
The disability was evaluated with the WHO-DAS II, which is a generic instrument designed by the World Health Organization as a measure of disability; it incorporates 6 dimensions of the functioning of the individual that define the disability construct: understanding and communication, ability to move in his environment, personal care, relationships with other people, activities of daily living and participation in society. It was obtained a score for each domain and a total value in a range from 0 to 100, from best to worst.7
The QL in the adult patients with moderate or severe haemophilia was evaluated using the QL Short Form-36 (SF-36) questionnaire that consists of 36 questions, which measure 8 dimensions of health (physical function, social function, physical performance, emotional performance, mental health, vitality, bodily pain and general health). The score is rated from 0 (worst health status) to 100 (optimal health status). The survey was applied through a personal interview. This questionnaire is validated in Colombia.8 In the children and adolescents between 8 and 18 years, was evaluated the KIDSCREEN 27, which is a generic instrument that measures 5 dimensions of HRQoL: (1) physical activity and health, (2) mood and feelings, (3) family life and free time, (4) social support and friends, and (5) school environment. The scores for each dimension are transformed into values with a mean of 50 and a standard deviation of 10; the higher scores indicate better QL and well-being. This questionnaire is also validated in Colombia.9
The pain was evaluated using the visual analog scale (VAS), which consists of a line of 0–10cm, with an end marked as «no pain» and another end that indicates “the worst pain imaginable”.10
The symptoms of depression were assessed with the Patient Health Questionnaire (PHQ-9), which is a self-report questionnaire designed to detect symptoms of depression in the past 2 weeks; it consists of 9 questions that are qualified with a score of 0–3, being zero never, and 3 almost every day; the total sum is obtained and is interpreted according to the resulting value: 1–4 minimal depression, 5–9 mild depression, 10–14 moderate depression, 15–19 moderately severe depression and 20–27 severe depression.11
Statistical methodsThe SPSS Stadistic 20 software was used. The quantitative variables were described by means of measures of central tendency, medians with their ranges or means with their standard deviations according to whether or not these variables had a normal distribution. The variables of QL of the SF36 and the KIDSCREEN-27 were described with means or medians with their measures of dispersion and were transformed into a scale from 0 to 100. The sample was divided into 2 groups according to the criteria for disease severity; in the first group the individuals with mild and moderate haemophilia, and in the second group the individuals with severe haemophilia, to compare the differences between groups in the different categories of the scale of QL, the 6-min walk test and the PHQ-9 depression scale. In addition, it was made the comparison of the categories of the QL scale with a group of healthy people from the city of Medellin, taking as reference 139 healthy subjects interviewed in the study of evaluation of the reliability of the SF-36 conducted by Lugo et al.8
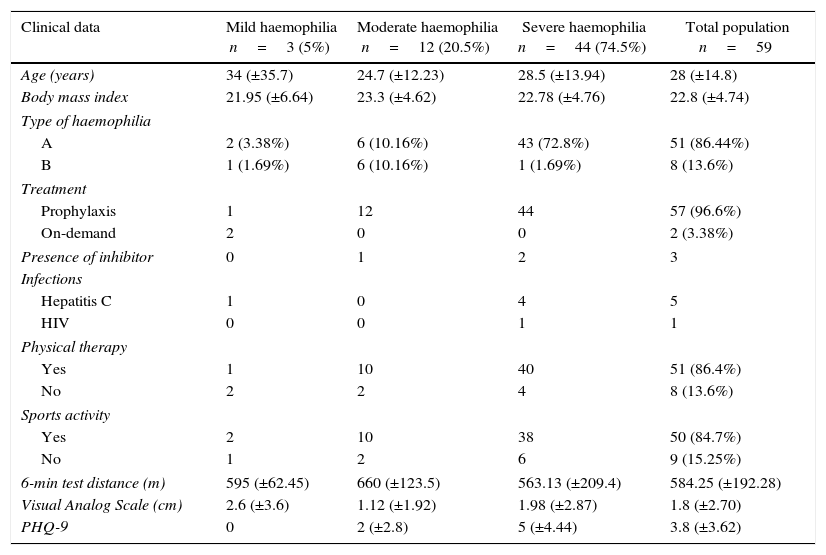
ResultsOf a sample of 60 patients, 59 accepted to participate in the study. The main clinical and demographic characteristics of the patients studied are shown in Table 1. Of the studied population, 35% were students, 12% were unemployed, 39% were employed, 8.5% were pensioners and the remaining 5% were patients under 2 years of age.
Clinical and demographic characteristics of the population.
| Clinical data | Mild haemophilia n=3 (5%) | Moderate haemophilia n=12 (20.5%) | Severe haemophilia n=44 (74.5%) | Total population n=59 |
|---|---|---|---|---|
| Age (years) | 34 (±35.7) | 24.7 (±12.23) | 28.5 (±13.94) | 28 (±14.8) |
| Body mass index | 21.95 (±6.64) | 23.3 (±4.62) | 22.78 (±4.76) | 22.8 (±4.74) |
| Type of haemophilia | ||||
| A | 2 (3.38%) | 6 (10.16%) | 43 (72.8%) | 51 (86.44%) |
| B | 1 (1.69%) | 6 (10.16%) | 1 (1.69%) | 8 (13.6%) |
| Treatment | ||||
| Prophylaxis | 1 | 12 | 44 | 57 (96.6%) |
| On-demand | 2 | 0 | 0 | 2 (3.38%) |
| Presence of inhibitor | 0 | 1 | 2 | 3 |
| Infections | ||||
| Hepatitis C | 1 | 0 | 4 | 5 |
| HIV | 0 | 0 | 1 | 1 |
| Physical therapy | ||||
| Yes | 1 | 10 | 40 | 51 (86.4%) |
| No | 2 | 2 | 4 | 8 (13.6%) |
| Sports activity | ||||
| Yes | 2 | 10 | 38 | 50 (84.7%) |
| No | 1 | 2 | 6 | 9 (15.25%) |
| 6-min test distance (m) | 595 (±62.45) | 660 (±123.5) | 563.13 (±209.4) | 584.25 (±192.28) |
| Visual Analog Scale (cm) | 2.6 (±3.6) | 1.12 (±1.92) | 1.98 (±2.87) | 1.8 (±2.70) |
| PHQ-9 | 0 | 2 (±2.8) | 5 (±4.44) | 3.8 (±3.62) |
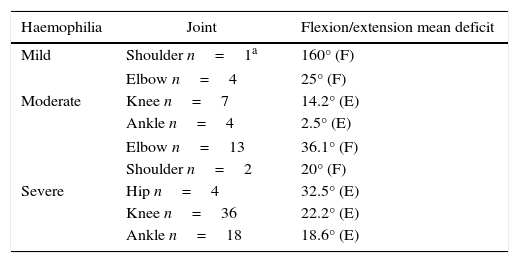
In the PHQ-9 scale, the patients with mild and moderate haemophilia had a mean score lower than 4, indicating that they had only minimal depression; and in the patients with severe haemophilia the mean score was 5 which reveals mild depression. Regarding the cardiovascular risk factors, 27.1% of patients had dyslipidemia, 20% overweight, 11.8% tobacco consumption, 8.5% arterial hypertension and 8.5% obesity. Only one patient reported consumption of marijuana. The greatest comorbidity was the haemophilic arthropathy, which was observed in 42 patients (71%). 89 affected joints were found in the following order: knee 48.3%, ankle 24.7%, elbow 19.1%, hip 4.5%, and shoulder 3.3%. There was only one patient with hip joint replacement. In Table 2 are shown the movement deficit according to the severity of the haemophilia and the distribution by joints.
Mean range of motion deficit.
| Haemophilia | Joint | Flexion/extension mean deficit |
|---|---|---|
| Mild | Shoulder n=1a | 160° (F) |
| Moderate | Elbow n=4 | 25° (F) |
| Knee n=7 | 14.2° (E) | |
| Ankle n=4 | 2.5° (E) | |
| Severe | Elbow n=13 | 36.1° (F) |
| Shoulder n=2 | 20° (F) | |
| Hip n=4 | 32.5° (E) | |
| Knee n=36 | 22.2° (E) | |
| Ankle n=18 | 18.6° (E) | |
86.4% of the population attended a physical therapy program led by a physiotherapist, in which they performed aerobic, stretching and strengthening exercises, with an average attendance of 4 times per week. 84% of the population reported doing physical activity (walking, cycling or swimming) during at least 30min, 3 or more times per week in the last month. Of the patients, 13.5% used walking aids and of them, 50% used walking sticks, 37.5% crutches, and 12.5% Canadian cane. The 6-min walk test was carried out in 55 of the 59 patients; the test was suspended in one patient due to severe knee pain and was not performed in 3 patients because they were under 2 years of age. The distance walked by 14 patients with mild to moderate haemophilia was 646.07 (SD 114.4) and the distance walked by 41 patients with severe haemophilia was 563.13 (SD 209.43).
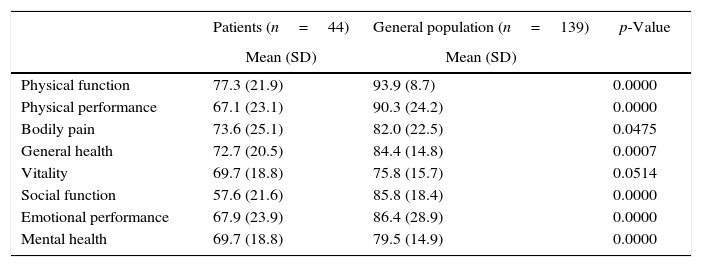
The scores of the SF-36 for the different dimensions of QL were evaluated in the patients with moderate or severe haemophilia, over 18 years of age, and compared with the general population of Medellin (Table 3). The scores found in the domains of vitality and bodily pain are similar in moderate and severe haemophilia; but in the rest of the domains, lover scores were found in severe haemophilia. The domains with the lowest scores corresponded to social function, physical performance and emotional performance, and the highest score was for physical function.
Scores of the different dimensions of the SF-36 in patients with moderate and severe haemophilia compared with a general population of Medellin (Colombia).
| Patients (n=44) | General population (n=139) | p-Value | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Physical function | 77.3 (21.9) | 93.9 (8.7) | 0.0000 |
| Physical performance | 67.1 (23.1) | 90.3 (24.2) | 0.0000 |
| Bodily pain | 73.6 (25.1) | 82.0 (22.5) | 0.0475 |
| General health | 72.7 (20.5) | 84.4 (14.8) | 0.0007 |
| Vitality | 69.7 (18.8) | 75.8 (15.7) | 0.0514 |
| Social function | 57.6 (21.6) | 85.8 (18.4) | 0.0000 |
| Emotional performance | 67.9 (23.9) | 86.4 (28.9) | 0.0000 |
| Mental health | 69.7 (18.8) | 79.5 (14.9) | 0.0000 |
The KIDSCREEN-27 questionnaire was completed by 9 patients with haemophilia and their scores were compared with those of the general population aged between 8 and 18 years. In the population with haemophilia the dimensions with the lowest mean scores corresponded to the domain of family life and free time (77.3) and of friends (79.6) and the highest mean score was in the domain school (86.7). The QL in patients with haemophilia and infections with HIV or hepatitis C showed low scores in the domains of physical function or general health. However, in the domain of emotional performance the patients with hepatitis C had scores above those of the general population without infections.
The WHODAS II questionnaire was filled out by 46 patients, since 13, because of their age, were not candidates to fill it out. The mean WHODAS score was 14.3 (SD 15.3). The worst performances were found in the domains of ability to move around with a score of 21.2 (SD 19.9) and participation in society with a score of 26.1 (SD 17.5). The domains with best performances were personal care with a score of 4.3 (SD 8.6) and understanding and communication with a score of 9.0 (SD 9.6).
DiscussionIn this study, the patients with haemophilia reported a HRQoL as high as that of the general Colombian population. No significant differences by age groups were found between patients under 19 years, 20–26 years, 27–37 years and older than 38 years. This is a finding similar to that described in other studies on QL in adults with haemophilia (Lindvall and Scalone).4,12
This sample of patients has higher scores in the domains of physical function, bodily pain and general health of the SF-36. Gringeri reported high scores in the domains of emotional performance and mental health, while Plug described the highest scores in social function and emotional performance.13,14 However, these results can be attributed to differences in the severity of the haemophilia, the presence of inhibitors, the working situation, the types of patients included in each study, or to health policies and cultural differences in each country, which lead to mixed results in the SF-36. Other aspects that might have contributed to the good scores of QL are that 96.6% of the patients received prophylaxis, which is associated with less joint damage, and that very few patients had the presence of inhibitors.15–17 The low frequency of inhibitors could have influenced that domains such as physical function (67±23) and general health (72.2±20.45) had scores higher than those reported by Scalone et al., because in that study they only included patients with inhibitors, situation that worsens the QL due to the progression of the arthropathy.12 In addition, the majority of the patients were linked to a program of physiotherapy or physical activity, which in turn contributes to a better physical health and a higher QL.18,19 Finally, another aspect that could have influenced the good QL scores is that the patients had only a minimal or mild depression, which impacts the QL.20
When comparing the QL with that of the general population of Medellin (Colombia), one of the domains with the lowest average score corresponded to the social function, indicating frequent interference with social activities, due to physical or emotional problems; which could be due to the frequent need to attend medical treatments and to the difficulties in accessing employment. The domains of physical function and general health were more affected in the patients with severe haemophilia than in those with mild and moderate haemophilia. This could be explained by the fact that in this group of patients there was a greater joint involvement, slightly higher levels of depression and that it is the group with more patients with hepatitis C infections, which have been associated with a lower QL.4
The QL scores obtained with the KIDSCREEN-27, were higher than those observed in other pathologies such as mental illnesses, congenital diaphragmatic hernia and in the long-term survivors of haemophilia.21,22 The results of the evaluation of the WHO DAS II showed that patients with haemophilia appear to have less disability than the reported for other chronic musculoskeletal diseases, such as ankylosing spondylitis.23 The most affected domains in this study were the ability to move around and the participation in society, information that correlates with the data of SF-36 in the domains of social function and physical function. In the studies of van Genderen and of Elander it was found association of the pain as a significant causal factor for functional limitation and deterioration in QL.24,25 However, due to the low levels of pain in the VAS found in the present study, it was considered that it did not influence the outcomes of functionality and HRQoL. In this study 12% of patients were unemployed, a percentage which is lower than that found in the study of Hartl et al. (34%), but slightly higher than the rate of unemployment in the general population of Colombia in 2014, which was 9.1%.26 A possible explanation is the difficulty that exists for the labor integration of a person with disability in a developing country like Colombia. The population under study had multiple cardiovascular risk factors that could be predictors of lower QL, as are also the presence of inhibitors and the severity of the haemophilia.27 Sedentary lifestyle in patients with haemophilia can influence their morbidity, acting as a risk factor for osteoporosis and cardiovascular diseases.28
Despite the full treatment based on prophylaxis and physical therapy, the patients with severe haemophilia, older than 38 years, had a greater number of affected joints, predominantly in lower limbs, situation reflected in a lower performance during the walk test. These characteristics are in accordance with the study published by Chen et al., who found that the limitation in the ranges of motion of the hip and knee are predictors of QL in individuals with haemophilia.5 This can be because this age group did not receive prophylactic treatment at an early age and had developed haemophylic arthropathy due to bleeding, mainly in the knees and ankles.
In the 6-min walk test, it was found a mean distance which is comparable to the distance expected for an adult without haemophilia (571±90m)29 even though 74% of the population was classified as having severe haemophilia and 71% of these patients had haemophilic arthropathy, with predominance in the joints involved in gait (knee, ankle and hip). The mean distance walked by the patients under 20 years of age was comparable to the distance expected for a child and adolescent without haemophilia (618±79m).30 One possible explanation is the treatment with prophylaxis since the first year of life for the early prevention of arthropathies. However, unlike our results, in a study with 47 children with haemophilia, Hassan concluded that they have a lower performance in the walk test compared with the healthy population.31 The maintenance of such functionality could be attributed to the fact that the majority of the population (84%) attended a physical therapy program with an additional home plan of exercise, and received prophylactic treatment. This approach was also suggested by Negrier et al., who mention the importance of performing physical therapy to prevent disability in people with haemophilia.18 Besides the described benefits of exercise in the population with haemophilia, physical activity in turn helps in the control of overweight, that predisposes to a worsening of the arthropathy and cardiovascular disease, and which in some cohorts of patients has been increasing.32 In the cohort of this study the incidence of overweight was very low.
Being an observational cross-sectional study, is not intended to establish causal relationships. The data obtained are useful to describe the characteristics of the individuals who suffer from the disease and to formulate hypothesis. The physical activity was determined by answering a single question but not filling out a structured questionnaire designed for this purpose as in the study of Niu.19 However, one of the strengths of this study was that the surveys were filled out in person, with the supervision of one of the researchers while attending treatment, unlike the study conducted by Williams et al., in which the surveys were sent, generating the possibility of biases due to the intervention of the parents.33
ConclusionThis group of patients with haemophilia reported a QL comparable to that of the Colombian general population without haemophilia. This finding reiterates the importance of the treatment with pharmacological prophylaxis and of the active participation of the patients with haemophilia in a rehabilitation program that promotes functional independence and a healthy lifestyle.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingThis research was financed with resources from the sustainability fund of the Health Rehabilitation Group of the University of Antioquia 2013–2014.
Conflict of interestThe authors declare they do not have any conflict of interest
Thanks to the administrative and healthcare staff of INTEGRAL IPS for the valuable collaboration in the data collection, to the Health Rehabilitation Group of the University of Antioquia and to the patients who are our reason for being.
Please cite this article as: Fuenmayor Castaño A, Jaramillo Restrepo M, Salinas Durán F. Calidad de vida en una población con hemofilia: estudio de corte transversal en un centro de tratamiento de hemofilia. Rev Colomb Reumatol. 2017;24:18–24.
