



Juvenile idiopathic arthritis (JIA) is one of the most common childhood chronic degenerative diseases causing serious sequelae such as disability and blindness with clinical course, prognosis and treatment for all different phenotypes.
ObjectiveTo determine the most common clinical subtypes of JIA in the rheumatology of a second level hospital care in northwestern Mexico.
Material and methodsUnder a cohort design were studied patients with JIA in rheumatology service. The classification into subtypes of the disease was performed by clinical and laboratory criteria issued by the ILAR. The frequency of the subtypes of JIA, as well as the latter's association with sociodemographic variables such as age and gender was measured.
ResultsFrom 35 patients with JIA predominance of female gender was 74% of the cases studied. The most affected age group was observed in patients between 10 and 12, most frequent subtypes was arthritis associated with enthesitis (40%) and poly articular JIA with positive rheumatoid factor (20%). Significant association between age and gender and gender cases and subtype of JIA found.
ConclusionsJIA cases presented at an earlier age in the male gender, unlike girls in which age presentation comes between 10 and 12 years.
La artritis idiopática juvenil (AIJ) es una de las enfermedades crónicas degenerativas más frecuentes en la infancia, ocasionando secuelas importantes tal como la discapacidad, ceguera con un curso evolutivo, pronóstico y tratamiento distinto para todos los fenotipos.
ObjetivoConocer los subtipos clínicos más frecuentes de AIJ en el Servicio de Reumatología de un hospital, de segundo nivel de atención, del noroeste de México.
Materiales y métodosBajo un diseño tipo cohorte se estudiaron pacientes con AIJ del Servicio de Reumatología. La clasificación en subtipos de la enfermedad se realizó mediante los criterios clínicos y de laboratorio emitidos por la ILAR. Se midió la frecuencia de los subtipos de AIJ, así como la asociación de estos con variables sociodemográficas como edad y género.
ResultadosSe estudiaron 35 pacientes con AIJ dentro de los cuales predominó el género femenino con el 74% de los casos. El grupo de edad más afectado se observó en los pacientes entre 10 y 12 años. Los subtipos de AIJ más frecuentes son la artritis asociada a entesitis (40%) y la AIJ poliarticular con factor reumatoide positivo (20%). Se encontró asociación significativa entre edad y género de los casos y género subtipo de AIJ.
ConclusionesLos casos de AIJ se presentan a más temprana edad en el género masculino, al contrario los femeninos se presentan en mayores de 9 años, esto nos podría orientar en el abordaje diagnóstico de pacientes con patología articular.
Juvenile idiopathic arthritis (JIA) is considered a chronic degenerative disease of unknown etiology, which leaves multiple important sequelae in the pediatric population, from disability to blindness and limitation in their basic activities of daily living.1,2 JIA, according to the International League of Associations for Rheumatology (ILAR), is defined as the tumefaction or limitation of motion of the joint accompanied by heat, pain or erythema, of unknown etiology, which begins before the age of 16 years and persists for at least 6 weeks with other conditions already excluded.3,4 The JIA is subdivided into different clinical subtypes, also proposed by the ILAR, which are JIA of systemic onset, oligoarticular, polyarticular with positive rheumatoid factor, polyarticular with negative rheumatoid factor, enthesitis-related arthritis, psoriatic arthritis and undifferentiated. In Mexico and Latin America there are not epidemiological studies that allow us to know the different clinical subtypes of JIA.5 Unlike other countries, such as those of Caucasian origin, where is documented that the one of oligoarticular origin is the most frequent, occurring in 30–40% of the cases.6 In other studies that have been conducted throughout the world, as for example in Zambia, it has been found that the polyarticular with positive rheumatoid factor and the oligoarticular are the most frequent.7 As for the gender, it is still predominant in women with a ratio of 3:1 with regard to men; and as for the age group, the most frequent age of presentation regarding the oligoarticular is between the first and the third year of life.1
Since JIA is cataloged as a chronic disease, its diagnosis can be delayed for the reason that the different clinical subtypes show great similarity and resemblance with other rheumatologic diseases and because it is a heterogeneous group which has specific characteristics that if not diagnosed can lead to complications and to a growing problem of disability, affecting the life expectancy in the patients, leading them to school absenteeism, so it is of utmost importance to study its epidemiology regarding the different clinical subtypes in order to provide timely treatment.4
The objective of this study was to know the frequency of the different clinical subtypes of JIA in pediatric patients of the Rheumatology Service of a hospital in Sonora, Mexico.
Materials and methodsPrevious authorization of the Local Committee of Ethics and Research in Health, a study under a cohort type design was conducted with pediatric patients under 16 years of age diagnosed with JIA in the Rheumatology Service of a hospital of second level of attention in Sonora, Mexico.
The diagnostic classification was carried out by an attending rheumatologist of the medical unit, using the diagnostic criteria proposed by the ILAR, according to the last consensus of Edmonton in 2001,5 in which are described the following exclusion criteria for JIA:
- a)
Psoriasis or antecedents of psoriasis in the patient or in a first-degree relative.
- b)
Arthritis in a male patient HLA B27+ that starts having symptoms after the age of 6 years.
- c)
Ankylosing spondyloarthritis, enthesitis-related arthritis, sacroiliitis, bowel inflammatory disease, Reiter's syndrome, acute anterior uveitis either in the patient or in a first-degree relative.
- d)
Positive rheumatoid factor (RF) (at least 2 determinations, with 3 months of interval).
- e)
Presence of systemic JIA in the patient.
The ILAR defines the different clinical subtypes of JIA as follows:
Oligoarticular JIA: defined as arthritis in 4 or less joints, is called persistent when it continues in 4 joints 6 months after the onset, and as extended when it occurs in more than 5 joints 6 months after the onset, with the exclusion criteria a, b, c, d and e.
Polyarticular JIA with positive rheumatoid factor: defined as arthritis in 5 or more joints in the first 6 months of the disease, with positive rheumatoid factor in 2 determinations with an interval of 3 months, with the exclusion criteria a, b, c and e.
Polyarticular JIA with negative rheumatoid factor: defined as arthritis in 5 or more joints in the first 6 months of the disease with negative rheumatoid factor, with exclusion criteria a, b, c, d and e.
Systemic-onset JIA: defined by the presence of arthritis in one or more joints, accompanied or preceded by fever of at least 2 weeks of duration, which is documented daily for at least 3 days, accompanied by one or more ore the following criteria: evanescent erythematous exanthema, generalized lymphadenopathy, hepatomegaly/splenomegaly, serositis, with the exclusion criteria a, b, c, d.
Enthesitis-related arthritis: defined by the presence of arthritis and enthesitis or the presence of arthritis or enthesitis with whichever of the 2 following antecedents: pain at the level of the sacroiliac joint or inflammatory pain in the lumbosacral area, positive HLA-B27, onset in a male patient aged 6 years or more, acute symptomatic anterior uveitis, presence of a first-degree relative with ankylosing spondylitis, enthesitis-related arthritis, inflammatory bowel disease with sacroiliitis, reactive arthritis or acute anterior uveitis with the exclusion criteria a, d, e.
Psoriatic arthritis: defined by the presence of arthritis and psoriasis or arthritis and at least two of the following antecedents: dactylitis, ungueal wells or onycholysis, psoriasis in a first-degree relative with the exclusion criteria b, c, d, and e.
The measured variables were the gender, the age at diagnosis, and the clinical subtype of JIA; these data were captured in a database in Excel format and SPSS version 18, carrying out the application of descriptive statistics through the distribution of frequencies and percentages of each of the categories of the variables, as well as measures of association between the clinical subtypes of JIA with gender and age; statistical significance was considered when the p-value was equal to or less than 0.05.
Study without risk to the patient according to the ethical norms of the General Health Law Regulation in the Field of Research for Health.
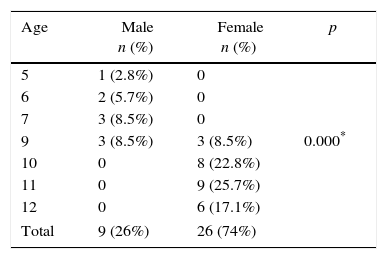
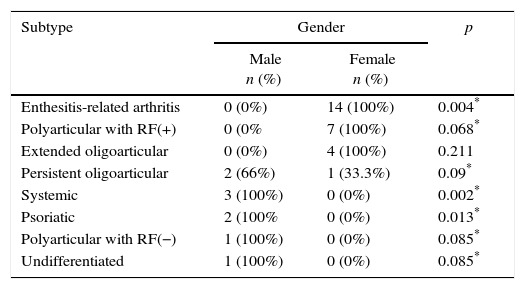
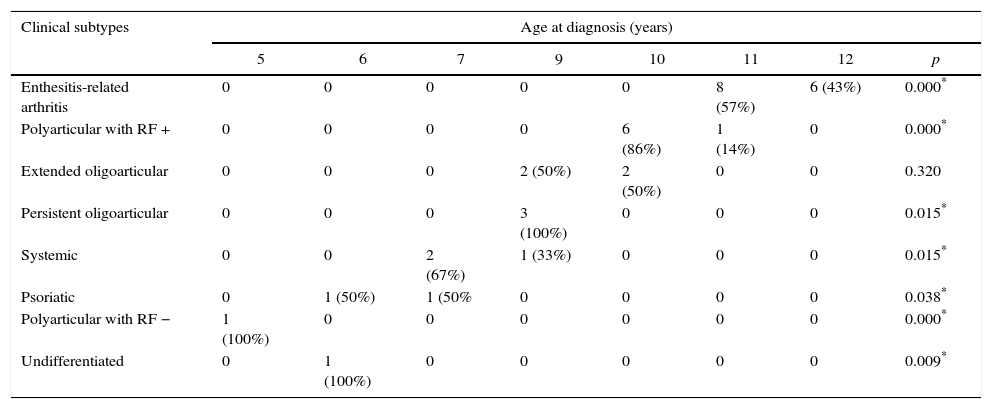
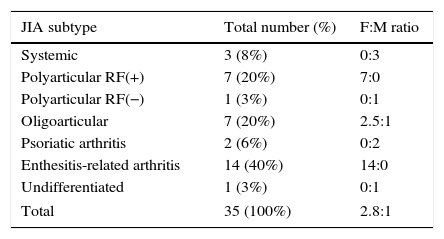
Results35 patients with diagnosis of JIA, treated in the Rheumatology Service were studied in the period comprised between 2012 and 2015. Among the results by gender the most affected was the female in 74% of cases (Table 1). The highest frequency of cases was observed in patients older than 10 years, corresponding to 65.7% of them (Table 2). The most frequent clinical subtype was the enthesitis-related arthritis, accounting for 40% of cases, followed by the polyarticular JIA with positive rheumatoid factor, accounting for 20% of cases (Table 3). It was observed that in the female gender the most frequent clinical subtypes were the enthesitis-related arthritis and the polyarticular with rheumatoid factor, with 14 and 7 cases, respectively, contrasting with the male gender, in which predominated the JIA, psoriatic arthritis and persistent oligoarticular with 3, 2 and 2 cases, respectively (Table 2). As for the association between age and the clinical subtypes of JIA, the enthesitis-related arthritis predominated in patients between 11 and 12 years of age, with 8 and 6 cases, respectively, and the polyarticular arthritis with positive rheumatoid factor in patients of 10 years of age (Table 3). The distribution of presentation according to gender showed a very wide variation depending on the JIA subtype, presenting in this series a female:male ratio of 14:0 in the enthesitis-related arthritis, 7:0 in the polyarticular with positive rheumatoid factor and 0:3 in the systemic (Table 4).
Description of patients with JIA from Northwestern Mexico by age and gender.
| Age | Male n (%) | Female n (%) | p |
|---|---|---|---|
| 5 | 1 (2.8%) | 0 | 0.000* |
| 6 | 2 (5.7%) | 0 | |
| 7 | 3 (8.5%) | 0 | |
| 9 | 3 (8.5%) | 3 (8.5%) | |
| 10 | 0 | 8 (22.8%) | |
| 11 | 0 | 9 (25.7%) | |
| 12 | 0 | 6 (17.1%) | |
| Total | 9 (26%) | 26 (74%) | |
JIA: juvenile idiopathic arthritis.
p: Chi-square.
Description of patients with JIA from Northwestern Mexico by gender and subtype n=35.
| Subtype | Gender | p | |
|---|---|---|---|
| Male n (%) | Female n (%) | ||
| Enthesitis-related arthritis | 0 (0%) | 14 (100%) | 0.004* |
| Polyarticular with RF(+) | 0 (0% | 7 (100%) | 0.068* |
| Extended oligoarticular | 0 (0%) | 4 (100%) | 0.211 |
| Persistent oligoarticular | 2 (66%) | 1 (33.3%) | 0.09* |
| Systemic | 3 (100%) | 0 (0%) | 0.002* |
| Psoriatic | 2 (100% | 0 (0%) | 0.013* |
| Polyarticular with RF(−) | 1 (100%) | 0 (0%) | 0.085* |
| Undifferentiated | 1 (100%) | 0 (0%) | 0.085* |
JIA: juvenile idiopathic arthritis, RF: rheumatoid factor.
p: Chi-square.
Description of patients with JIA from Northwestern Mexico by age at diagnosis and clinical subtypes.
| Clinical subtypes | Age at diagnosis (years) | |||||||
|---|---|---|---|---|---|---|---|---|
| 5 | 6 | 7 | 9 | 10 | 11 | 12 | p | |
| Enthesitis-related arthritis | 0 | 0 | 0 | 0 | 0 | 8 (57%) | 6 (43%) | 0.000* |
| Polyarticular with RF + | 0 | 0 | 0 | 0 | 6 (86%) | 1 (14%) | 0 | 0.000* |
| Extended oligoarticular | 0 | 0 | 0 | 2 (50%) | 2 (50%) | 0 | 0 | 0.320 |
| Persistent oligoarticular | 0 | 0 | 0 | 3 (100%) | 0 | 0 | 0 | 0.015* |
| Systemic | 0 | 0 | 2 (67%) | 1 (33%) | 0 | 0 | 0 | 0.015* |
| Psoriatic | 0 | 1 (50%) | 1 (50% | 0 | 0 | 0 | 0 | 0.038* |
| Polyarticular with RF − | 1 (100%) | 0 | 0 | 0 | 0 | 0 | 0 | 0.000* |
| Undifferentiated | 0 | 1 (100%) | 0 | 0 | 0 | 0 | 0 | 0.009* |
JIA: juvenile idiopathic arthritis, RF: rheumatoid factor.
p: Chi square.
Frequency of subtypes of patients with JIA from Northwestern Mexico and distribution of presentation according to the gender n=35.
| JIA subtype | Total number (%) | F:M ratio |
|---|---|---|
| Systemic | 3 (8%) | 0:3 |
| Polyarticular RF(+) | 7 (20%) | 7:0 |
| Polyarticular RF(−) | 1 (3%) | 0:1 |
| Oligoarticular | 7 (20%) | 2.5:1 |
| Psoriatic arthritis | 2 (6%) | 0:2 |
| Enthesitis-related arthritis | 14 (40%) | 14:0 |
| Undifferentiated | 1 (3%) | 0:1 |
| Total | 35 (100%) | 2.8:1 |
JIA: juvenile idiopathic arthritis; F:M: female:male; RF: rheumatoid factor.
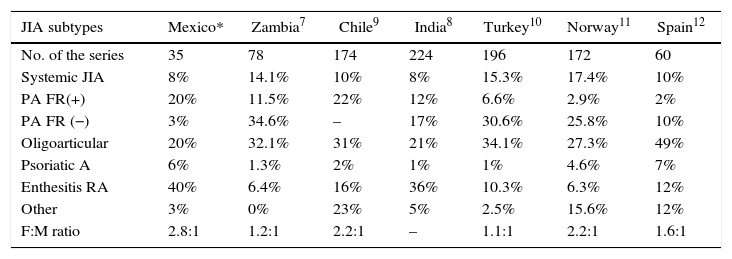
JIA represents a disease that causes disability and sequelae, and therefore, its diagnosis in a timely manner is of utmost importance in order to be able to distinguish the subclassification, since each one has a different prognosis, despite all of them have a chronic evolution. Regarding the epidemiology, in this cohort, there is similarity in terms of the most affected gender compared with studies published in South America and Europe,8–10 predominating in this study the female gender with 74% of the cases; in relation to the most frequent clinical subtypes, series published in Africa, South America and Europe7–11 report the oligoarticular subtype as the one of most frequent presentation, in contrast with the results of our study in which we found enthesitis-related arthritis and polyarticular arthritis with positive rheumatoid factor as the most frequent clinical subtypes. Statistically significant association was found between the age of onset, the gender and the JIA subtype; in the patients of female gender the disease began between 10 and 12 years of age in 100% of cases, in contrast to the population of male gender, in which the onset of the disease occurred between 5 and 9 years of age. The most frequent clinical subtypes in this series: enthesitis-related arthritis, and polyarticular with positive rheumatoid factor, have a more aggressive behavior with functional limitation in many cases leading to disability and deformity, due to early joint damage as reported in the “Clinical patterns of juvenile idiopathic arthritis in Zambia” study12 where it was possible to demonstrate that the polyarticular presentation with positive rheumatoid factor was the most frequent by 34.6%, finding ocular affections with presence of uveitis as the most frequent chronic complication. When comparing the distribution of subtypes with those of other series published worldwide, the highest frequency in European and Asian countries corresponds to the oligoarticular subtype,8–11 in African series predominate the polyarticular subtypes,7 and the enthesitis-related predominates in our series and in the one reported in India12 (Table 5).
Distribution of the subtypes and ratio of affection according to the gender of patients with JIA in series of different countries.
| JIA subtypes | Mexico* | Zambia7 | Chile9 | India8 | Turkey10 | Norway11 | Spain12 |
|---|---|---|---|---|---|---|---|
| No. of the series | 35 | 78 | 174 | 224 | 196 | 172 | 60 |
| Systemic JIA | 8% | 14.1% | 10% | 8% | 15.3% | 17.4% | 10% |
| PA FR(+) | 20% | 11.5% | 22% | 12% | 6.6% | 2.9% | 2% |
| PA FR (−) | 3% | 34.6% | – | 17% | 30.6% | 25.8% | 10% |
| Oligoarticular | 20% | 32.1% | 31% | 21% | 34.1% | 27.3% | 49% |
| Psoriatic A | 6% | 1.3% | 2% | 1% | 1% | 4.6% | 7% |
| Enthesitis RA | 40% | 6.4% | 16% | 36% | 10.3% | 6.3% | 12% |
| Other | 3% | 0% | 23% | 5% | 2.5% | 15.6% | 12% |
| F:M ratio | 2.8:1 | 1.2:1 | 2.2:1 | – | 1.1:1 | 2.2:1 | 1.6:1 |
Enthesitis RA: enthesitis-related arthritis, JIA: juvenile idiopathic arthritis; Psoriatic A: psoriatic arthritis; F:M ratio: female:male ratio; PA FR (+): polyarticular with positive rheumatoid factor; PA FR (−): polyarticular with negative rheumatoid factor.
The important points to be investigated in future studies would be: Which are the risk factors for the development of JIA in the Mexican population in contrast with other developing countries? or Why the clinical subtypes are different from those published in series from other countries? To what extent would influence the genetic, nutritional and environmental antecedents of our context?
In this group of patients we observed that those who have enthesitis-related JIA; generally have first-degree relatives with spondyloarthropathies that occur more in the male gender (father), which is frequent in this geographical area. However, this theory cannot be corroborated since there are few reports in Mexico that describe the frequency of presentation of the subtypes of the disease and the various risk factors to which they could be associated.
Our country has a very large territorial area, with big differences among the populations according to the geographical regions; it would be convenient to compare our cases with those which exist in other regions of the country and, in turn, with Latin American countries in order to have a much broader panorama of the presentation of the disease in our country and continent.
ConclusionsIn this case series the most affected gender is the female, with a female:male ratio of 2.8:1; the most frequent clinical subtype is the enthesitis-related arthritis with 40% of cases, followed by the polyarticular with positive rheumatoid factor with 20%. As for the age of presentation, it prevailed between 10 and 12 years. An important association that was observed and which could be useful for the clinician when suspecting a disease of rheumatologic origin is that in the female gender the age of onset was between 10 and 12 years, in contrast to the male gender, in which the onset occurred between 2 and 5 years of age. It is important to recognize the epidemiological and clinical pattern of the cases of JIA at the local level in order to facilitate the diagnosis and approach of these cases, detect complications early and avoid the appearance of sequelae that affect the quality of life of this group of patients.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingResources from the Hospital General Regional Numero Uno (HGR no. 1) of the IMSS in Ciudad Obregón, Sonora, Mexico.
Conflict of interestThe authors declare they do not have any conflict of interest.
To the nursing staff of the Service of Rheumatology, Pediatrics and Clinical Records for the facilities provided. To Dr. Mónica López Morales for the support and impulse to the research process.
Please cite this article as: Arreguin-Reyes R, Valle-Leal J, Lozano Rentería L, Medina-Valenton E, Álvarez Bastidas L. Descripción de una cohorte de pacientes de artritis idiopática juvenil en el estado de Sonora, México. Rev Colomb Reumatol. 2016;23:236–241.
