



Morbid obesity is an epidemic and complex disease which imposes a multidisciplinary approach. Laparoscopic sleeve gastrectomy has become a frequent procedure given its efficacy and safety compared to other surgical options. However, it isn’t free from complications. Lax gastric fixation or incorrect positioning of the stomach during surgery can result in early gastric outlet obstruction caused by a volvulus-like mechanism by rotation of the stomach around its anatomic axes. This report refers to two cases of post sleeve gastric torsion resulting in persisting vomiting after initiating oral intake. The diagnosis was confirmed by upper gastrointestinal-contrast study and gastroscopy. In both cases, a fully covered self-expandable metallic stent was inserted which prompted the gastric lumen to become permeable resulting in symptomatic resolution. The stents were removed endoscopically after two and three months. Beyond more than three years of follow-up, the patients remain asymptomatic and no recurring “stenosis” was noticed. In these cases the use of fully covered self-expandable metallic stents demonstrated to be effective and safe in the treatment of post sleeve gastric torsion.
A obesidade mórbida é uma doença epidémica complexa, que impõe uma abordagem multidisciplinar. A gastrectomia vertical laparoscópica tornou-se um procedimento frequentemente utilizado dada a sua eficácia e segurança em comparação com outras opções cirúrgicas. Contudo não é isenta de complicações. A fixação gástrica mais laxa ou o posicionamento incorreto do estômago durante a cirurgia pode resultar em obstrução gástrica precoce após a cirurgia, que é provocada por um mecanismo semelhante ao do volvo – por rotação do estômago em torno do seu próprio eixo anatómico. Apresentam-se dois casos de torção gástrica pós gastrectomia tubular, resultando em vómitos persistentes depois do início da dieta oral. O diagnóstico foi confirmado por estudo contrastado gastrointestinal e gastroscopia. Em ambos os casos, foram colocadas próteses metálicas auto-expansíveis totalmente cobertas, restituindo a permeabilidade do lúmen gástrico com resolução sintomática. As próteses foram removidas endoscopicamente ao fim de 2 e 3 meses. Após mais de 3 anos de seguimento, os doentes permanecem assintomáticos e não se verificou “estenose” recorrente. Nestes casos, o uso de próteses metálicas auto-expansíveis totalmente cobertas demonstrou ser eficaz e seguro no tratamento da torção gástrica pós gastrectomia tubular.
Morbid obesity is an epidemic and complex disease which imposes a multidisciplinary approach. Laparoscopic sleeve gastrectomy (LSG) has become a frequent procedure given its efficacy and safety compared to other surgical options. The most common complications are staple line bleeding, strictures that are usually located at the middle or distal portion of the residual stomach, and leaks, which are the most severe and life-threatening.1 Lax gastric fixation or incorrect positioning of the stomach during surgery can result in early gastric outlet obstruction (EGOO) caused by a volvulus-like mechanism by rotation of all or part of the stomach around its anatomic axes2 (Fig. 1). We have managed two cases of EGOO, 10 and 24 days after LSG. Both patients suffered from persisting vomiting after initiating oral intake.
2Case report
Patient one: A 24-year-old male, longstanding morbidly obese, body mass index (BMI) of 41.8kg/m2, underwent a LSG. The patient was hospitalized for five days with no signs or symptoms of postoperative adverse events. Ten days after LSG, he was admitted with persisting vomits.
Patient two: A 25-year-old obese female, with a BMI of 32.3kg/m2, underwent a LSG. There were no technical adverse events. The immediate postoperative period was incident-free and she was discharged four days after surgery. She was admitted with alimentary vomits 20 days after having been discharged.
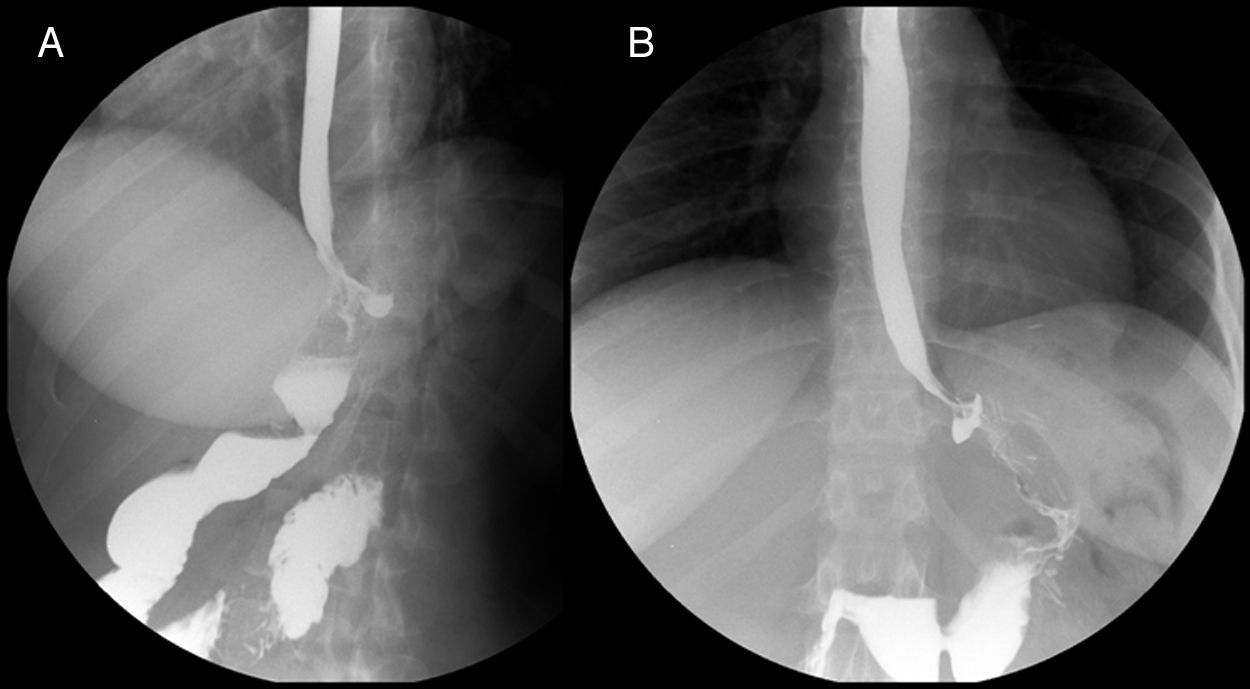
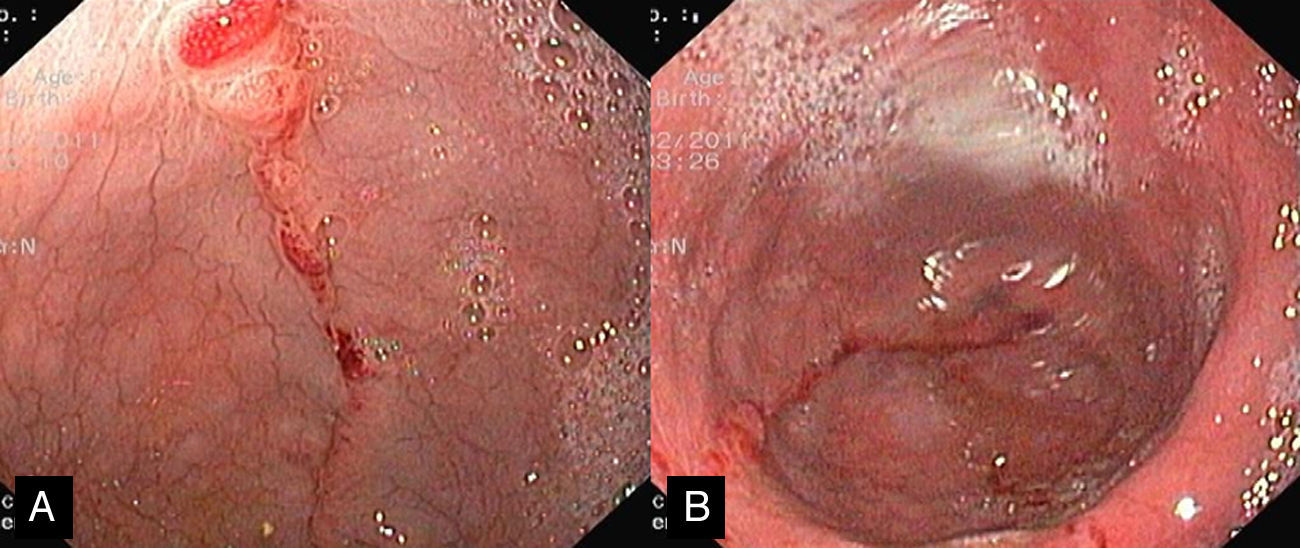
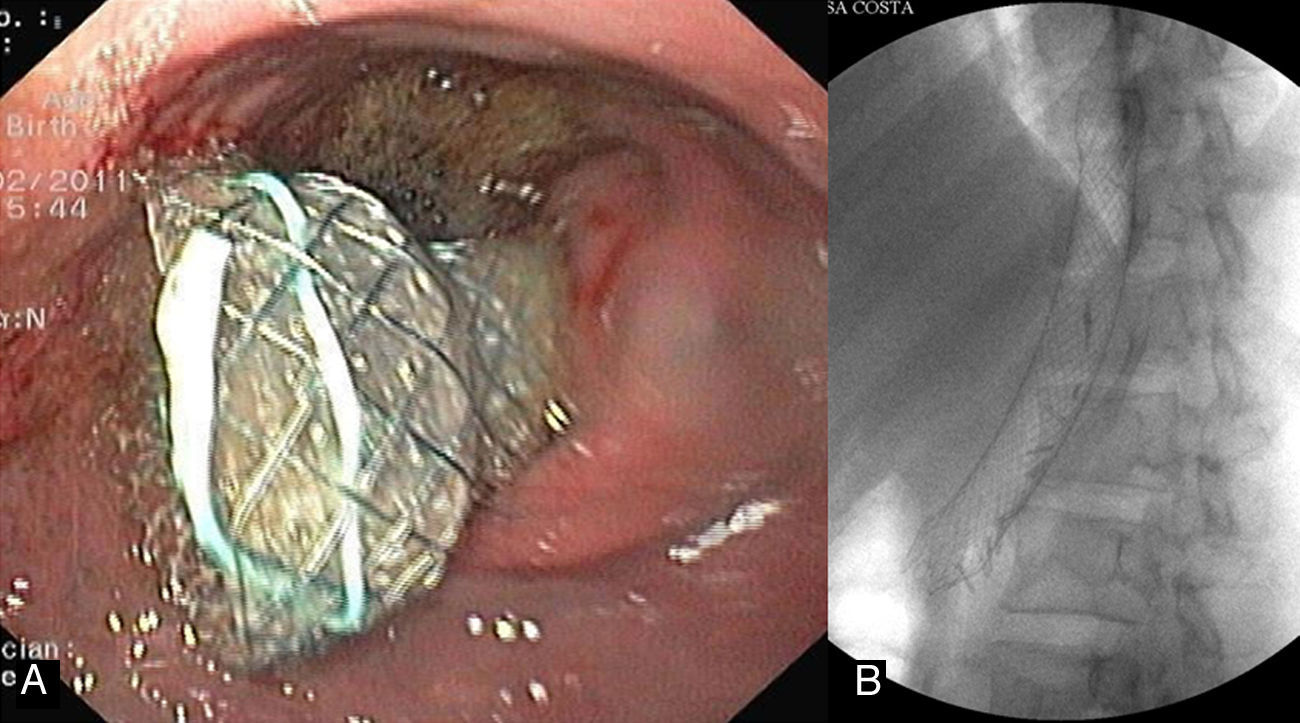
Gastrografin fluoroscopy revealed gastric “stenosis” in both cases, due to torsion over the main axis of the stomach (Fig. 2). The upper endoscopy showed a widened gastric lumen followed by a rotated segment located at mid-body, resulting in a short “stenosis” (Fig. 3). A fully covered self-expandable metallic stent was used in both cases (Taewoong Niti-S® 28/80mm – patient 1; Boston Scientific Wallflex® 23/105mm – patient 2; Fig. 4). In both cases, fixation with endoscopic clips was not required nor any other sort of stent fixation device. The endoscopic procedure prompted the gastric lumen to become permeable resulting in immediate symptomatic resolution. Both patients were discharged on the following day.
.")
 followed by a rotated segment located at mid-body of the stomach (B).")
 and fluoroscopic (B) view of fully covered self-expandable metallic stent in situ.")
After two and three months (patient 1 and patient 2 respectively) the stents were removed by endoscopy on an ambulatory basis. The stents were correctly positioned and no signs of stent migration were noticed. Rat tooth grasping forceps were used to gently pull the proximal end of the stent. Stent removal was easy and only mild and self-limited bleeding was noticed after the procedure.
After over three years of follow-up, the patients remain asymptomatic and no recurring “stenosis” was noticed.
3DiscussionLSG has emerged as a reproducible successful and efficient surgical technique for long-term weight loss stability with regression of most major associated comorbidities.3 The complication rate for LSG has been described to be 2.9 up to 15.3%.4 Obstruction after laparoscopic sleeve gastrectomy is rare but requires early diagnosis and treatment due to a significantly increased morbidity.
The obstruction can result from an anatomical stricture of the gastric tube or from gastric tube's functional obstruction due to twisting by a volvulus-like mechanism. The twisting may occur by misalignment of the staples in the same plane or by the indentation of the incisura within the gastric lumen, which creates a flap valve producing a functional EGOO. Another cause of obstruction is adhesions of the gastric serosa thappening later on.3
Few reports of EGOO after LSG related to this mechanism have been published.2–7 In one of these cases,6 a Polyflex® covered esophageal stent (Boston Scientific, Natick, MA, USA) was inserted under fluoroscopic guidance. However the stent migrated up into the esophagus and required surgical removal. The remaining cases were surgically sorted out.
In these cases the use of fully covered self-expandable metallic stents demonstrated to be effective and safe in the treatment of post sleeve gastric torsion. EGOO is a functional gastric tube obstruction that may recur. However, in the reported cases the patients remained asymptomatic during a follow-up of at least three years.
The excellent short-term outcome was expected given that the stents insertion prompted the gastric lumen patency. The good long-term outcome was less expectable and was probably due to the induction of ulceration and fibrosis in the gastric torsion inducing a permanent gastric tunnel.
In case of therapeutic failure these patients would be candidates to surgery aiming to convert the sleeve gastrectomy into a gastric bypass.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Conflict of interestThe authors have no conflicts of interest to declare.
