




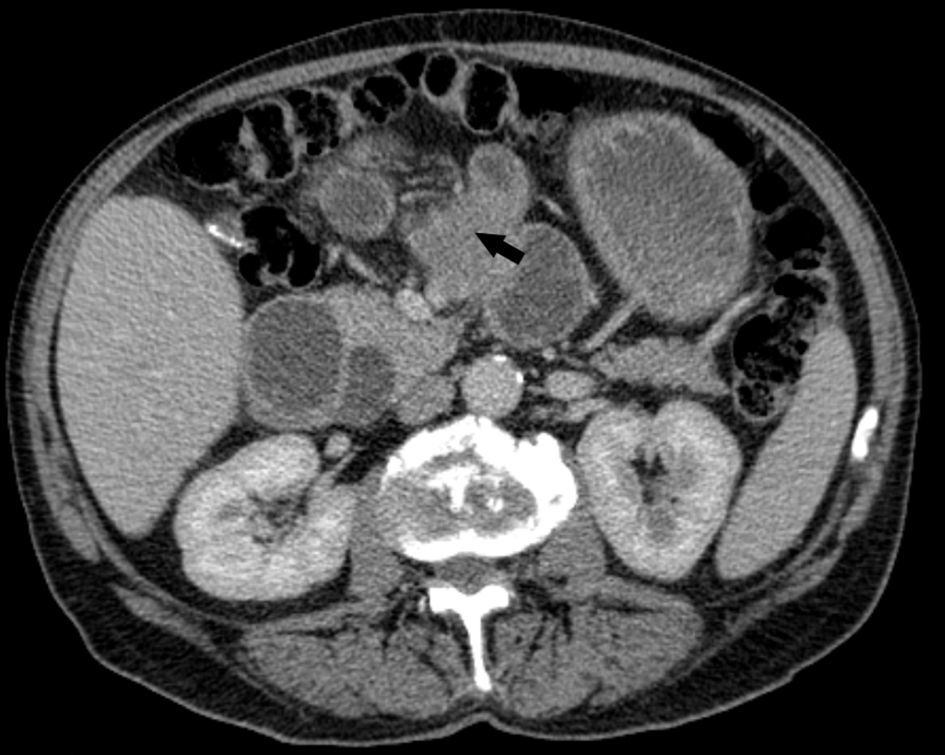
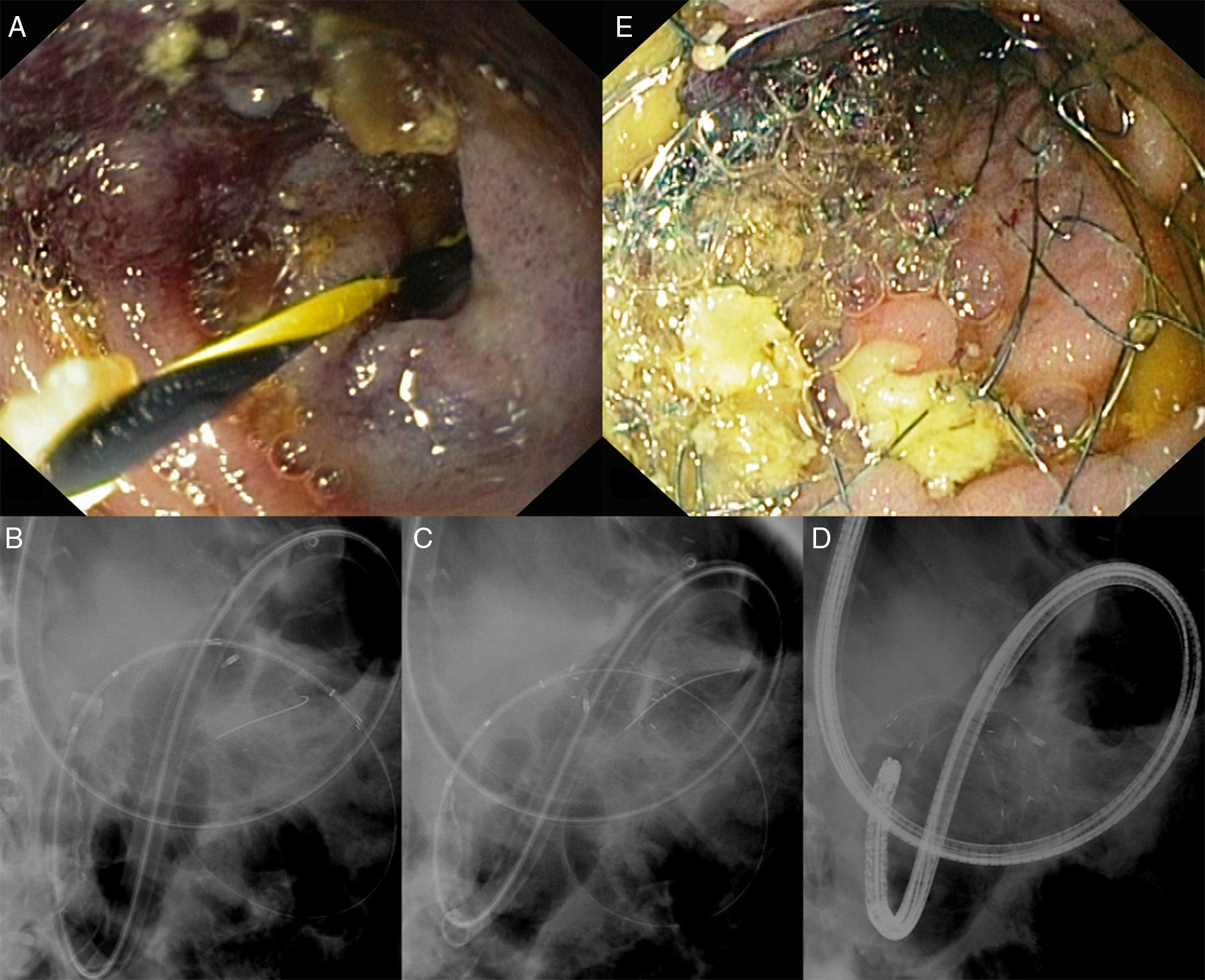
A 75-year-old man with past history of surgical resection 21 months ago and adjuvant chemotherapy of a cholangiocarcinoma that was followed by palliative chemotherapy for peritoneal carcinomatosis 4 months ago, presented with a 1-week history of persistent vomiting and abdominal pain. Computed tomography revealed a peritoneal implant of 42mm, confirmed histologically, (Fig. 1) leading to extrinsic compression and obstruction of the proximal jejunum near the ligament of Treitz with pronounced gastric and duodenal distension. The patient was referred for palliative stenting using single-balloon enteroscopy (SBE; SIF-Q180; Olympus, Tokyo, Japan), after an unsuccessful attempt to reach the stenosis with a gastroscope and a colonoscope. The SBE was advanced through the stenosis and its distal end was marked with a clip. After positioning the overtube (ST-SB1, Olympus) at the proximal limit of the stenosis, a 0.035-inch guidewire was advanced through the stenosis (Fig. 2A) and the enteroscope was removed. A non-covered self-expandable metallic stent (SEMS; Hanarostent, DNZL-20-110-230, M.I. Tech Co., Seoul, South Korea) was then easily advanced over-the-wire (OTW) through the overtube (Fig. 2B) and subsequently deployed under fluoroscopic guidance (Fig. 2C) while the overtube was slightly pulled back. After stent insertion (Fig. 2D and E), the patient tolerated oral diet and was discharged two days later and remains asymptomatic 3 months later.
 causing extrinsic compression and obstruction of a jejunal loop.")
 Endoscopic image showing the guide-wire passing through the jejunal stenosis. (B) Fluoroscopic image showing the advancement of the SEMS over the wire and through the overtube. (C) Fluoroscopic image revealing the release of the SEMS while the overtube was slightly pulled back. (D) Fluoroscopic image depicting proper placement of the SEMS in the stenosis. (E) Endoscopic image, after releasing the stent and reintroducing the enteroscope, showing the stenosis with the SEMS.")
(A) Endoscopic image showing the guide-wire passing through the jejunal stenosis. (B) Fluoroscopic image showing the advancement of the SEMS over the wire and through the overtube. (C) Fluoroscopic image revealing the release of the SEMS while the overtube was slightly pulled back. (D) Fluoroscopic image depicting proper placement of the SEMS in the stenosis. (E) Endoscopic image, after releasing the stent and reintroducing the enteroscope, showing the stenosis with the SEMS.
In the past few years, the development of deep enteroscopy enabled diagnostic evaluation of the small-bowel.1,2 Moreover, several endoscopic therapeutic techniques were adapted to deep enteroscopy.1,2 Nevertheless, palliative stenting of malignant stenoses located beyond the reach of conventional endoscopy is still challenging.1 Enteral stents have a delivery system larger and shorter than the working channel of the enteroscope preventing the use of the through-the-scope technique, which allows a easier stent deployment in stenoses located distant from the insertion route.1,3–5 A modified OTW technique using an overtube may prevent looping of the delivery system, allowing placement of SEMS with deep enteroscopy in the small-bowel.1,4,5

