



In recent years, the introduction of high-resolution units has increased the importance of the adequate training of endocrinologists new to thyroid gland ultrasound, including the performance of associated techniques, mainly fine needle aspiration biopsy (FNAB). In addition to the necessary theoretical training, this complex technique undoubtedly requires practicing time in order for it to be performed with maximum guarantees and safety for the patient, as well as with the greatest possible effectiveness. However, to date few publications have addressed the existing learning curve of fine needle aspiration biopsy of the thyroid gland. The article published by Penín et al.,1 which sheds some more light on this subject and has allowed the learning curve to be characterized, is therefore to be recognized and applauded. However, given our experience, some questions may be raised and comparisons can be made with the learning curve observed at our center based on a retrospective study compiling the pathology findings from patients subjected to ultrasound-guided FNAB performed by the same endocrinologist in the period between September 2014 and June 2016.
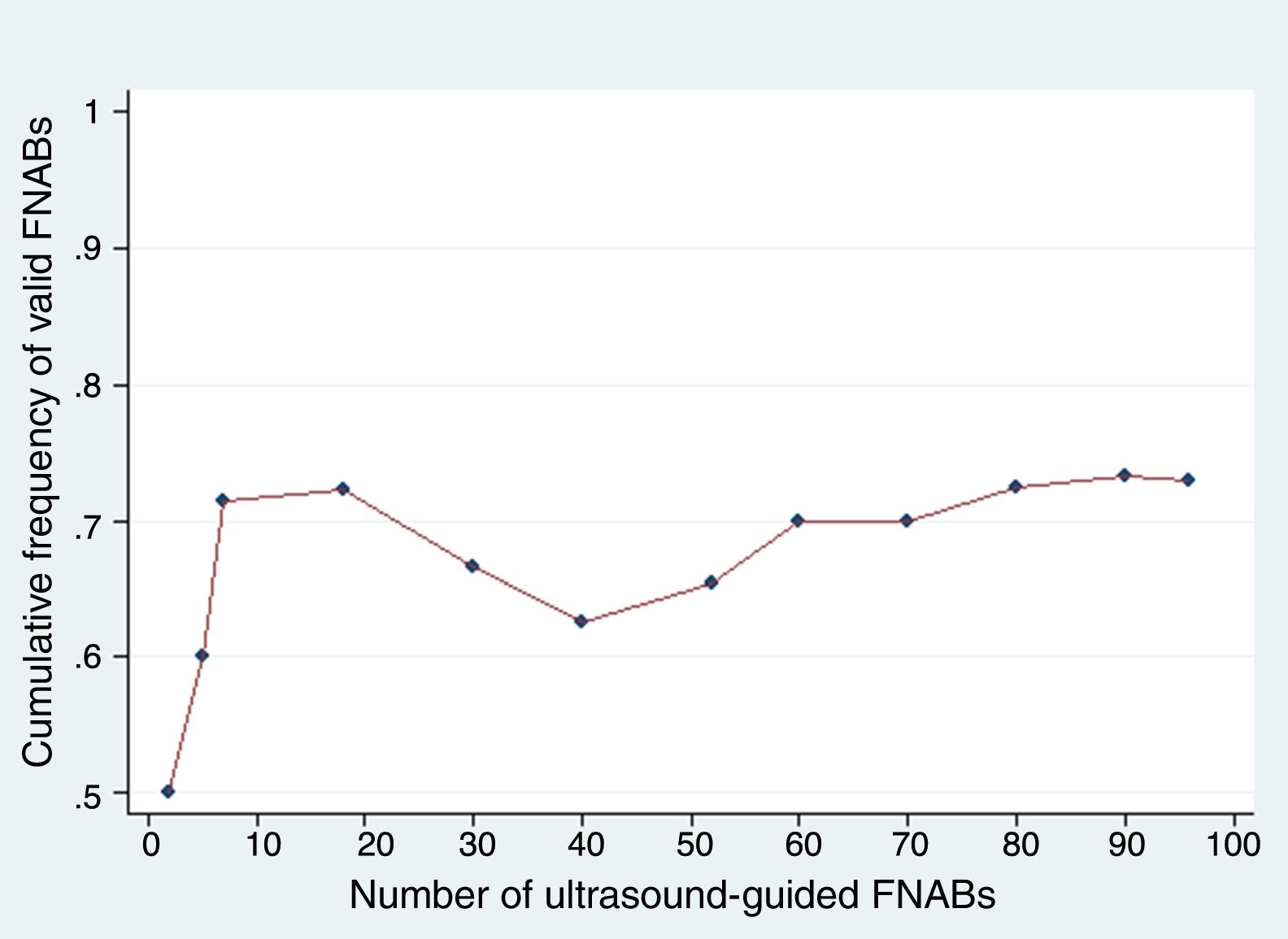
The need for intensive training in performing this diagnostic technique was already known, because its main disadvantage and limitation is the incidence of inadequate and non-evaluable samples for diagnosis, which under optimum conditions should not exceed 20%.2 In this regard, up to three punctures in the same FNAB procedure are needed to ensure the maximum diagnostic yield according to the existing guides and related articles.3 Based on the analysis of the results of the article, we established a cut-off point defined as 60 ultrasound-guided FNAB procedures with two punctures in each procedure, to secure a learning curve affording a percentage diagnostic rate of over 80%, or similar to the performance of the reference expert endocrinologist. A study was made comparing three blocks of 20 punctures each to determine whether there were differences between the first and last blocks and between the two endocrinologists. We considered that it might also be interesting to perform a cumulative frequency analysis of valid FNABs to assess not only improvement in performance, but also the maintenance of the success rate. This, in turn, would allow us to identify the moments in which significant fluctuations can be seen. An example of this is shown in Fig. 1.

Despite the limited literature, the existing studies disagree on the number of ultrasound-guided FNAB procedures required to secure optimum sample diagnostic yield.4
In turn, we feel that there may be some ethical concerns in the study carried out by Penin et al., because it involved four punctures targeted to the same nodule in each patient, corresponding to two punctures per ultrasound-guided FNAB procedure performed by the expert endocrinologist and the novice. As previously mentioned, there are articles and guidelines that recommend three punctures per FNAB procedure in order to minimize the percentage of inadequate samples.3 However, in the abovementioned article each patient was subjected to an additional puncture. This diagnostic technique is not without possible complications, and although the problems are usually mild and infrequent, the fact of subjecting a patient to additional punctures may lead to an increased risk of complications.
With regard to our own experience, a description is provided below of the learning curve obtained in our center in a high-resolution thyroid nodule unit. It should be noted that we only analyzed punctures in patients who had not undergone prior punctures performed by the endocrinologist, thereby discarding second punctures made after an invalid puncture result (Bethesda I) versus the rest (Bethesda II or higher).
Fig. 1 shows that the curve stabilizes in our study from puncture 70–80, and continues to show an improvement between puncture 60 and the subsequent punctures. Of note is the fact that the percentage of FNAB procedures with cumulative valid results did not reach 80% (the percentage being around 73%).
A number of limitations may be found in our sample, the most important being the diversity of pathologists analyzing the samples (6 in total). This constituted one of the strengths of the paper published by Penín et al., controlling for one of the potential effect-modifying factors, though no differences were noted in our analysis due to the diversity between pathologists and the cytology results.
Please cite this article as: Marco-Alacid C, López-Merseguer M, Tolosa-Torréns M. Consideraciones en relación a la curva de aprendizaje de la punción-aspiración con aguja fina de tiroides y experiencia propia en nuestro centro. Endocrinol Diabetes Nutr. 2018;65:420–421.